CROSS-REFERENCES TO RELATED APPLICATIONS
-
The present application is a continuation application of U.S. application Ser. No. 11/022,172 filed Dec. 22, 2004 which claims priority under Title 35, United States Code, .sctn.119 to provisional application U.S. Patent application Ser. No. 60/532,764 filed Dec. 24, 2003.
FIELD OF INVENTION
-
The present invention relates to compositions and methods for treating cardiac (brady-) arrhythmias, and more particularly to systems and methods involving the application of gene and cell therapy to treat cardiac pacing dysfunction.
BACKGROUND OF THE INVENTION
-
In a normal human heart, cardiac contraction is initiated by the spontaneous excitation of the sinoatrial (“SA”) node that is located in the right atrium. The electrical current generated by the SA node travels to the atrioventricular (“AV”) node where it is then transmitted to the bundle of His and Purkinje network, which branches in many directions to facilitate coordinated contraction of the left and right ventricles.
-
The cellular basis for the aforementioned electrical impulse is the action potential (AP). The AP is conventionally divided into five phases (phases 0-4) in which each phase is defined by the cellular membrane potential and the activity of potassium, sodium, chloride, and calcium ion channel proteins that affect that potential. These channels, embedded in cell membranes, allow for electrical impulses to occur as they permit charged ions to rush through them. Propagation of electrical activity from an individual cardiac cell to surrounding cardiac tissue takes place through gap junctions, small pore-like structures that connect cardiac muscle cells to each other. The role of ion channels in cardiac electrical conduction is analogous to electrical conduction in other tissues such as skeletal muscle.
-
Some channels or gates have their own “non-provoked” rhythmic excitation also known as automaticity. The generation of cardiac automaticity is based on a complex interplay between at least four different channels of cationic (positive ion) nature: T- and L-type calcium channels, a cation channel named If, and potassium channels. The If channel has been termed the pacemaker channel. If channels have unique properties such as: 1) If channels open upon membrane hyperpolarization; 2) If channels allow for mixed cation current (Na+ and K+); 3) cyclic AMP (cAMP-cyclic adenosine monophosphate which serves as an intracellular messenger molecule) binds to the cytoplasmic site of the channel thereby accelerating its activation kinetics and shifting the voltage dependence of the cell to more positive voltages; and lastly 4) If channels are susceptible to blockade by extracellular Cs+ (cesium ion). The genes responsible for the If channel currents have recently been identified and belong to the HCN (hyperpolarization-activated cyclic nucleotide-gated) family. Four different isoforms have been identified in vertebrates (HCN1, HCN2, HCN3 and HCN4) and all except HCN3 have been found in the heart. HCN3 is specifically expressed in neurons.
-
HCN channels directly interact with intracellular cAMP so that an increase in cAMP levels results in increased If and more positive activation potentials. This increase thereby accelerates the heart rate (HR) in response to sympathetic stimulation. In contrast, muscarinic stimulation slows the heart rate in part due to a decrease in cAMP levels and a resulting reduction of If and more negative activation potentials. Ludwig, A. et al.; “Two pacemaker channels from human heart with profoundly different activation kinetics.” EMBO J. (1999) 18 (9):2323-2329. The importance of the HCN genes in regulating heart rate has recently been shown in a patient who suffered from mutation in his HCN4 gene. This mutation consisted of a complete deletion of the C-terminus of the gene which included the cAMP binding domain. This patient suffered from symptomatic bradycardia and an electronic pacemaker needed to implanted. These mutations were recreated in vitro experiments, and the mutated channel was expressed in a cell line. The mutated HCN4 channel was completely inresponsive to cAMP. See, J Clin Invest. 2003 May: 111(10):1537-45.
-
HCN1 is primarily expressed in the brain and shows little dependence on cAMP. HCN1 is also expressed in the rabbit SA node and displays properties of brain h-channels in that it has a short AP. HCN2 and HCN4 are predominantly expressed in the heart, as well as in the brain, and produce currents similar to If. HCN1 is the fastest activating channel (25-300 ms), followed by HCN2 and HCN3 (180-500 ms), and lastly HCN4 (a few hundred ms to seconds). All four subunits induce pacemaker current similar to If if the units are expressed in heterologous expression systems. In addition, the four isoforms can interact with one another to form tetramers (couplings whereby the two isomers join to create a functionally different structure). The heteromerization of the isoforms changes pacemaker electrophysiology via altered activation kinetics (e.g., allows for modulation (increase or decrease) of heart rate). (Much B et al. J of Biol Chem; 44 (31): 43781-43786). While the exact stoichiometry of the heteromerized HCN channels has not been described yet, it is considered that these channels may form heteromers with a 3:1 ratio, but ratios of 1:1 or 1:3 are also possible as the HCN channels are known to form tetramers. In related rod photoreceptor cyclic nucleotide-gated channels, an asymmetrical stoichiometry of the two subunits present in the tetramers of 3:1 was determined. Zhong H et al. Nature 2002; 420: 193-196. Weitz D et al. Neuron 2002; 36: 881-889. Zheng J et al. Neuron 2002; 36: 891-896.
-
To avoid misunderstandings due to different naming of the same proteins, isoform nomenclature for the mouse brain is as follows: HCN1 corresponds to HAC2 (mBCNG-1), HCN2 corresponds to HAC1 (mBCNG-2) and HCN3 corresponds to HAC3 (mBCNG4).
-
In certain diseased states, the heart's ability to pace properly is compromised. For example, failure of SA nodal automaticity, resulting in an insufficient number of electrical impulses emanating from the SA node, is the most common cause of bradyarrhythmias (heart rhythm that is too slow). If slowing is enough so that the resultant heart rate is insufficient to meet the body's demand, symptoms result. Symptomatic bradycardia originating from the sinus node is part of a clinical syndrome characterized by brady- and tachyarrhythmias originating from a diseased sinus node, commonly referred to as sick sinus syndrome. Clinically, sick sinus syndrome is a very common problem and accounts for approximately 70% of all pacemaker implants in the general population. Other bradyarrhythmic disease states due to slowed or absent impulse propagation include the various degrees of AV block (e.g. 1st, 2nd, or 3rd). Tachyarrhythmias (heart rhythm that is too fast) and fibrillation are also a concern. These conditions present major problems ranging from cost of treatment to diminished quality of life and even death.
-
Currently, bradyarrhythmias are most commonly treated by the implantation of (exogenously driven) electronic pacemaker. While improving the lives of many patients, implantable pacemakers have a limited lifetime and consequently may expose a patient to multiple surgeries to replace the implantable pacemaker. Biological methods of influencing the pacing rate of cardiac cells, however, have recently been developed, including the use of various drugs and pharmacological compositions. Developments in genetic engineering have resulted in methods for genetically modifying cardiac cells to influence their intrinsic pacing rate. For example, U.S. Pat. No. 6,214,620 describes a method for suppressing excitability of ventricular cells by over-expressing (e.g. K+ channels) or under-expressing certain ion channels (e.g. Na+ and Ca2+ channels). PCT Publication No. WO 02/087419 describes methods and systems for modulating electrical behavior of cardiac cells by genetic modification of inwardly rectifying K+ channels (specifically, IK1) in quiescent ventricular cells.
-
Of particular import to those who suffer from bradyarrhythmias due to insufficient production of If; PCT Publication No. WO 02/098286 describes methods for regulating pacemaker function of cardiac cell via modulation of HCN channels ( HCN 1, 2, or 4 isoforms). See also U.S. Patent Application No. 2002/0187948, PCT Application No. WO 02/087419 A2, U.S. Patent Application Publication No. US 2002/0155101A1 and U.S. Pat. No. 6,214,620.
-
Still, there is a need to improve current methods of using HCN to treat cardiac patients and create pacemaker current capable of being turned on, off and modulated as well as having the capability to react to physiological stimuli to ultimately restore physiological heart rates in patients suffering from arrhythmias.
SUMMARY OF THE INVENTION
-
The present invention is directed to methods of using HCN genes, variants or subunits thereof to treat a cardiac pacing dysfunction. The various isoforms of HCN that include HCN1, HCN2, HCN3 and HCN4, and modified HCN genes (e.g. truncated HCN4) may be combined to induce a pacemaker current and treat a patient in need thereof. In addition, HCN genes can be combined with other types of genes including genes that promote beta-adrenergic receptors or genes that suppress Ik1 current to treat cardiac pacing dysfunction.
-
Specifically, genes that suppress or block IK1 may be combined with HCN genes including variants or subunits of the HCN isoforms. This combination may prevent an instable cycle length created by the HCN gene alone. Further, one or more HCN genes may be combined together with other channel-focused genes that encode beta-adrenergic receptors to create biopacemakers with physiological heart rate and rate responses. Modifying the ratios and doses of the aforementioned genes can modify the gene-based biological pacemaker to induce different pacemaker currents.
-
The subject invention includes a method of using HCN3 alone or in combination with other isoforms of HCN and/or other genes to treat cardiac pacing dysfunction. The subject invention further includes a method of using a truncated HCN4 gene alone or in combination with other isoforms and/or variants of HCN and/or other genes to treat cardiac pacing dysfunction.
-
Genes may be delivered to the heart via a construct that is transfected into a cell in vitro, or via gene therapy in vivo. The HCN gene induces a slow depolarizing diastolic pacemaker current in atrial, ventricular or conductive tissue.
-
Further, genes may be introduced into cells via a viral vector or comparable delivery system. The genes can be transfected into target cells such as endogenous cardiac cells (e.g., atrial or ventricular myocytes, cells of the conduction system including SAV, AVN and Purkinje system, cardiac fibroblasts, etc.), stem cells (e.g. autologeous, allogeneic or xenogeneic adult, fetal or embryonic stem cells), myoblasts or other cells. Endogenous cells such as atrial or ventricular cells are transfected using local delivery of a genetic therapy via catheter, direct injection, or equivalent delivery means. Other cells may be transfected outside of the body and then delivered to the heart using a catheter or equivalent means. For example, genetically modified cells may be delivered to the heart via self-fixating scaffolds.
-
Finally, by altering the molecular composition of the gene construct (e.g., adding certain promoters or regulatory elements to the HCN gene), the location, amount and characteristics of induced pacemaker current may be modified. Consequently, methods of subject invention may be specific for targeted cells instead of accidentally influencing, for example, a non-cardiac cell (e.g., a brain cell). Also, the pacemaker current can be regulated by controlling the expression of the transfected gene using, for example, pharmaceuticals that are directed towards the promoters of the transfected gene.
-
The foregoing has outlined rather broadly the features of the present invention in order that the detailed description of the invention that follows may be better understood. Additional features and advantages of the invention will be described hereinafter which form the subject of the claims of the invention.
BRIEF DESCRIPTION OF THE DRAWINGS
-
For a more complete understanding of the present invention, and the advantages thereof, reference is now made to the following description taken in conjunction with the accompanying drawings, in which:
-
FIG. 1 is a diagram of a human heart.
-
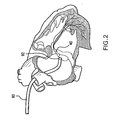
FIG. 2 is a diagram of the right side of a heart in which a guiding catheter is positioned for delivery of the genetic construct of the invention.
-
FIG. 3 depicts an example of a generic viral vector expression cassette that includes a promotor, regulatory elements and a transgene.
-
FIG. 4 depicts an example of a specific viral vector expression cassette that includes a promotor, regulatory element and the HCN3 gene for transfection.
-
FIG. 5 is a recording of induced pacemaker current obtained from experiments using human embryonic kidney cells transfected with human HCN3 gene.
-
FIG. 6 is a recording of spontaneous action potential cycle lengths induced by HCN, Ik1-block and a combination HCN expression and Ik1-block.
-
FIG. 7 depicts an image showing green fluorescent expression four weeks after injection of recombinant adeno-associated virus encoding enhanced green fluorescent protein (rAAV-eGFP) in canine myocardium.
-
FIG. 8 depicts the complete length of native HCN4 compared to truncated HCN4.
-
FIG. 9 depicts the expression data of two trials of HCN3 as transfected Human Embryonic Kidney (HEK) 293 cells by Quantitative Real-time Polymerase Chain Reaction (Q RT PCR).
-
FIG. 10 depicts immunolabeling (c-myc antibody) of HEK 293 cells co-transduced cells with AAV1/2 HCN4tr and AAV1/2-eGFP.
-
FIG. 11 depicts eGFP-labeling of the HEK 293 cells shown in FIG. 11 co-transduced cells with AAV1/2-HCN4tr and AAV1/2-eGFP.
-
FIGS. 12A-D depict whole cell voltage clamp current traces of If recorded from HL-5 cells.
-
FIGS. 13A-B depict comparisons of activation kinetics of If recorded in control and cardiac HL-5 cells transfected with rAAV-HCN4tr.
-
FIG. 14 depicts HCN4 whole cell voltage-clamp electrophysiology data recorded from HEK 293 cells transfected with full plasmid HCN4.
-
FIG. 15 depicts HCN4 whole cell voltage-clamp electrophysiology data recorded from HEK 293 cells transfected with truncated plasmid HCN4.
-
FIG. 16 depicts HCN4 whole cell voltage-clamp electrophysiology data recorded from HEK 293 cells transfected with truncated HCN4-myc AAV.
-
FIG. 17 depicts HCN3 whole voltage-clamp electrophysiology data recorded from HEK 293 cells transfected with HCN3 AAV.
-
FIG. 18 depicts a pulse protocol for determining activation kinetics.
-
FIG. 19 depicts current recordings obtained using the protocol of FIG. 18 from truncated hHCN4 in pIRES2-EGFP.
-
FIG. 20 depicts another pulse protocol for determining reversal potential.
-
FIG. 21 depicts current recordings obtained using the protocol of FIG. 19 from truncated hHCN4 in pIRES2-EGFP.
-
FIG. 22 depicts voltage-dependent activation curves for HCN4 and HCN4 truncated.
-
FIG. 23 depicts time constants of activation τact at certain activation voltages for HCN4 and HCN4 truncated.
-
FIG. 24 depicts the reversal potential for both the full-length and truncated hHCN4.
DETAILED DESCRIPTION OF THE INVENTION
-
The subject invention is directed to methods of treating patients with cardiac dysfunction by administering one or more HCN genes or variants thereof, alone or in combination with other genes.
DEFINITIONS
-
The following definitions are provided to facilitate an understanding of the invention.
-
“AAV” is an adeno-associated virus vector. These viruses cause no known disease in humans, hold long-term expression, and theoretically integrate at specific sites.
-
“AdV” is an adenovirus vector. These viruses cause the common cold. They have efficient entry into most cell types and can infect non-dividing cells. For gene therapy, these vectors are made replication-deficient by specifically deleting viral genes (e.g., E1, E2, E3 and/or E4). These genetically engineered vectors do not cause the common cold, although immune reactions to viral genes expressed in host cells can be observed.
-
“cDNA” includes all nucleic acids that share the arrangement of sequence elements found in native mature messenger ribonucleic acid (RNA) species, where sequence elements are exons (e.g., sequences encoding open reading frames of the encoded polypeptide) and 3′ and 5′ non-coding regions. Normally mRNA species have contiguous exons, with the intervening introns removed by nuclear RNA splicing, to create a continuous open reading frame encoding the polypeptide of interest.
-
“Channel protein” or “Ion channel protein” refers to proteins that transportions across cell membranes.
-
“Chromosomes” are DNA molecules and their associated proteins. A gene is a unit of inheritance which occupies a specific locus on a chromosome and which has a specific sequence of nitrogenous bases. A genome is the total set of genes carried by an organism or cell.
-
“Construct” is a recombinant nucleic acid, generally recombinant DNA that has been generated for the expression of a specific nucleotide sequence(s), or is to be used in the construction of other recombinant nucleotide sequences.
-
“DNA,” deoxyribonucleic acid, has a sugar group (deoxyribose) with the following nucleotide bases: adenine (A), guanine (G), thymine (T), and cytosine (C). RNA, ribonucleic acid, has ribose as the sugar group, and the same nucleotide bases, except uracil (U) replaces thymine. A single strand of DNA has a sequence of bases A, G, T, and C. When forming a DNA double-helix, for example, this secondary structure is held together by hydrogen bonds between bases on the neighboring strands. Note that in such base pairing, A always bonds to T and C always bonds to G.
-
“Coding sequence” refers to a nucleic acid sequence that is transcribed (in the case of DNA) and translated (in the case of mRNA) into a polypeptide, in vitro or in vivo, when placed under control of the appropriate regulatory sequences.
-
“Gap junction” refers to small pore-like proteins that connect cardiac muscle cells to each other.
-
“Gene” is a piece of DNA that encodes genetic traits and information.
-
“Gene cloning” is the process of identifying the gene responsible for a particular disease and synthesizing copies of it for use in treatment.
-
“Gene expression” describes the process by which a gene's coded information is converted into the structures present and operating in the cell. Expressed genes include those that are transcribed into mRNA and then translated into protein and those that are transcribed into RNA but not translated into protein (e.g., transfer and ribosomal RNAs).
-
“Gene therapy” is a technique for correcting genetic problems by introducing a “correct” copy of the gene into the patient's cells to compensate for their own defective gene. An alternative definition for “gene therapy” is the introduction of recombinant DNA into mammalian cells with the goal of modulating protein function (e.g., by expressing, replacing or suppressing a protein) for therapeutic purposes.
-
“Genome” is the complete set of genes in the chromosomes of each cell.
-
“Lentivirus” is a virus, such as HIV, that incorporates its passenger genes into non-dividing cells.
-
“Liposome” is a cationic lipid that is an artificially produced non-viral molecule vector that may transmit DNA to a cell. Sometimes this method is called facilitated DNA.
-
“Messenger ribonucleotide acid” or “mRNA” refers to RNA that serves as a template for protein synthesis.
-
“Nucleic acid” is a linear polymer of nucleotides (as in an oligomer, but longer) linked by 3′,5′ phosphodiester linkages.
-
“Nucleoside” is a purine or pyrimidine base linked glycosidically to ribose or deoxyribose.
-
“Nucleotide” is a phosphate ester of a nucleoside.
-
“Oligonucleotide” is a linear sequence of nucleotides, or mers, joined by phosphodiester bonds.
-
“PCR,” or “polymerase chain reaction,” is a system for in vitro amplification of DNA wherein two synthetic oligonucleotide primers, which are complimentary to two regions of the target DNA (one for each strand) to be amplified, are added to the target DNA in the presence of excess deoxynucleotides and Taq polymerase, a heat stable DNA polymerase. In a series of temperature cycles, the DNA is repeatedly denatured, annealed to the primers, and a daughter strand extended from the primers. As the daughter strands act as templates in subsequent cycles, amplification occurs in an exponential fashion. Since “traditional” PCR is a semi-quantative method at best, more recently, real-time (RT) PCR has been developed to allow quantification of RNA or DNA.
-
“Plasmid DNA” is circular DNA molecules typically found in bacteria.
-
“Polynucleotide” is an oligonucleotide, nucleotide, and fragments or portions thereof, as well as to peptide nucleic acids (PNA), fragments, portions or antisense molecules thereof, and DNA or RNA of genomic or synthetic origin which can be single- or double-stranded, and represent the sense or antisense strand.
-
“Promoter” is a minimal nucleotide sequence sufficient to direct transcription in a recombinant cell. “Promoter” is also meant to encompass those elements sufficient for promoter-dependent gene expression controllable for cell-type specific, tissue-specific or inducible by external signals or agents. Such elements may be located in the 5′ or 3′ regions of the native gene (e.g., enhancer elements).
-
“Regulatory gene or agent” is a gene with the primary function of controlling the rate of synthesis of the products of one or several other genes or pathways.
-
“Retrovirus” is a class of viruses that infects cells by inserting its own DNA into the genetic material of a host cell.
-
“Stem cells” are cells having the ability to divide for indefinite periods in culture and to give rise to specialized cells. Adult stem cells are undifferentiated cells found in a differentiated tissue that can renew itself and, with certain limitations, differentiate to yield all the specialized cell types of the tissue from which it originated. For example, adult resident cardiac stem cells have been identified. Bone marrow stromal cells are stem cells found in bone marrow that generate bone, cartilage, fat, and fibrous connective tissue. Mesenchymal stem cells are cells from the immature embryonic connective tissue. A number of cell types come from mesenchymal stem cells, including cardiac myocytes. Another example of adult stem cells are skeletal muscle progenitor cells. Embryonic stem cells are primitive, undifferentiated cells from the embryo that have the potential to become a wide variety of specialized cell types.
-
“Transformation”, “transduction” or “transfection” refers to a permanent or transient genetic change induced in a cell following incorporation of a new nucleic acid (e.g., DNA or RNA exogenous to the cell). Genetic change can be accomplished either by incorporation of the new nucleic acid into the genome of the host cell, or by transient or stable maintenance of the new DNA as an episomal element.
-
“Transformed cell”, “transfected cell” or “transduced cell” refers to a cell into which (or into an ancestor of which) has been introduced, by means of recombinant DNA techniques, a DNA molecule encoding a protein of interest.
-
“Transgene” is a gene that has other DNA inserted into it.
-
“Vector” refers to a means of transfecting cells with genetic material either in vivo or in vitro. Many such vectors are modified viruses.
The Cardiac Conduction System
-
FIG. 1 is a schematic diagram of a right side of a heart having an anterior-lateral wall peeled back to present a portion of a heart's intrinsic conduction system and chambers of a right atrium (“RA”) 16 and a right ventricle (“RV”) 18. Pertinent elements of the heart's intrinsic conduction system, illustrated, in FIG. 1, include a SA node 30, an AV node 32, a bundle of His 40, a right bundle branch 42, left bundle branches (not shown) and Purkinje fibers 46. SA node 30 is shown at a junction between a superior vena cava 14 and RA 16. An electrical impulse initiated at SA node 30 travels rapidly through RA 16 and a left atrium (not shown) to AV node 32. At AV node 32, the impulse slows to create a delay before passing on through a bundle of His 40, which branches, in an interventricular septum 17, into a right bundle branch 42 and a left bundle branch (not shown) and then, apically, into Purkinje fibers 46. Following the AVN delay, the impulse travels rapidly throughout RV 18 and a left ventricle (not shown). Flow of the electrical impulse described herein creates an orderly sequence of atrial and ventricular contraction and relation to efficiently pump blood through the heart. When a portion of the heart's intrinsic conduction system becomes dysfunctional, efficient pumping is compromised, potentially leading to symptoms which range from mild to life-threatening.
-
Typically, a patient, whose SA node 30 has become dysfunctional, may have an implantable pacemaker system implanted wherein lead electrodes are placed in an atrial appendage 15. The lead electrodes stimulate RA 16 downstream of dysfunctional SA node 30 and the stimulating pulse travels on to AV node 32, bundle of His 40, and Purkinje fibers 46 to restore physiological contraction of the heart. If a patient has a dysfunctional AV node 32, however, pacing in atrial appendage 15 will not be effective, since it is upstream of a block caused by the damage. In this situation, multiple chamber pacemaker system may be implanted (e.g. one pacemaker lead in the atrium, one in the ventricle), allowing for coordinated electromechanical activation of atria and ventricles.
-
Pacing at the bundle of His 40 provides the advantage of utilizing the normal conduction system of the heart to carry out ventricular depolarizations. In other words, stimulation provided at the bundle of His will propagate rapidly to the entire heart via the right bundle 42, the left bundle (not shown), and the Purkinje fibers. This provides synchronized and efficient ventricular contraction that is not replicated when the pacing is performed from the apex of the right ventricle because the electrical activity propagates via slowly conducting myocardial tissue as opposed to the rapidly conducting Purkinje network. By implanting biological pacemakers in or close to areas of physiological conduction (e.g. SAN, atrial septum, AVN, HIS bundle, Purkinje system), this principle could be applied to the current invention.
-
On the cellular level, electrical wave propagation occurs when cardiac cells allow a controlled flow of ions across the membranes through ion channels. This ion movement across the cell membrane results in changes in transmembrane potential (i.e., depolarization), which is a trigger for cell contraction. The heart cells can be categorized into several cell types (e.g. atrial, ventricular, etc.) and each cell type has its own characteristic variation in membrane potential. For example, ventricular cells have a resting potential of −85 mV. In response to an incoming depolarization wave front, these cells fire an action potential with a peak value of −20 mV and then begin to repolarize, which takes −350 ms to complete. In contrast, SA nodal cells do not have a stable resting potential and instead begin to spontaneously depolarize when their membrane potential reaches −50 mV. Cells, such as SA nodal cells, that do not have a stable resting transmembrane potential, but instead increase spontaneously to the threshold value, causing regenerative, repetitive depolarization, are said to display automacity.
-
Cardiac muscle cells are structurally connected to each other via small pore-like structures known as gap junctions. When a few cardiac cells depolarize, they act as a current source to adjacent cells causing them to depolarize as well; and these cells in turn impose on further adjacent cells, and so on. Once depolarization begins within a mass of cardiac cells, it spreads rapidly by cell-to-cell conduction until the entire mass is depolarized causing a mass of cardiac cells to contract in a coordinated fashion.
-
The cells in the SA node are specialized pacemaker cells and have the highest firing rate. Depolarization from these cells spreads across the atria. Since atrial muscle cells are not connected intimately with ventricular muscle cells, conduction does not spread directly to the ventricle. Instead, atrial depolarization enters the AV node, and after a brief delay, is passed on to the ventricles via the bundle of His and Purkinje network, initiating cellular depolarization along the endocardium. Depolarization then spreads by cell-to-cell conduction throughout the entire ventricular mass.
-
The SA node's unique cells include a combination of ion channels that endow it with its automacity. Some of the unique features of the SA node cells, relative to other myocardial cells, include the absence of Na+ channels (INa) and inwardly rectifying K+ (IK1) channels. In the absence of sodium current, the upstroke of SA node action potential is primarily mediated by L-type Ca2+ channels (IcaL). SA node cells do not have a stable resting potential because of their unique distribution of ion channels (e.g. lack of IK1, HCN expression). Consequently, they begin to depolarize immediately after the repolarization phase of the action potential is complete. The maximum diastolic potential for SA node cells is approximately −50 mV compared to −78 mV and −85 mV for atrial and ventricular cells, respectively. The slow depolarization phase is partially mediated by activation of the hyperpolarization-activated cyclic nucleotide channels (If current) and T-type Ca2+ channels and deactivation of slow and rapid potassium channels (IKs and IKr, respectively), in conjunction with a lack of IK1 current which serves in non-automatic atrial and ventricular cardiac myocytes as a membrane potential stabilizing current. The rate of pacemaker discharge in the SA node in a normally functioning heart is approximately in the range of about 60 to 100 beats per minute at rest.
-
In a heart with dysfunctional SA node pacemaker function, the other structures of the heart with intrinsic pacemaking activity can take over the pacing function. The ectopically-driven escape rhythm produced by these structures, however, is slow (bradycardia) and normally not sufficient to support normal circulation (symptomatic bradycardia). A symptomatic bradycardia can manifest itself as syncope (temporary loss of consciousness) which may be life-threatening.
-
A method of the present invention includes genetically modifying the atrial cells, ventricular cells or cells of the cardiac conduction system, such as the Purkinje fibers, to modify the electrophysiology and pacing rate to resemble more closely the electrophysiology and pacing rate of the specialized pacemaker cells of the troubled SA or AV nodes. FIGS. 14 through 17 depict HCN3 and HCN4 single cell patch-clamp electrophysiology data for cells transduced with constructs containing HCN3, HCN4 and HCN4 truncated (“HCN4tr”).
-
Native cells could also be transduced in a similar fashion. Subsequently their previously stable resting potential would be characterized by slow repeated phase 4 depolarizations and ultimately leading as the dominant pacemaker site of the heart. Similarly, cells could be stabily transduced with the constructs described in FIGS. 14-17, and then transplanted to the myocardium. These cells could, once electrically coupled to native cardiac cells, depolarize the native cells and induce biological pacemaking as described with the more classical gene therapy approach. If the transplanted cells are of a cardiac phenotype (such as c-kit positive cardiac stem cells), then these cells could act as pacemaker cells themselves since they would express the necessary ion channel proteins for action potential generation as well as electrical coupling (e.g. gap junction channel proteins).
Selection of Gene Construct
-
The human SA node does not consist of a group of uniform sinoatrial node cells embedded in atrial muscle. Instead, the SA node is a heterogeneous tissue with multiple cells types and a complex structure. From the periphery to the center of the SA node, there is a gradient in action potential shape, pacemaking, ionic current densities and connexin expression. In short, the SA node is a complex structure that, when afflicted with any level of dysfunction, may need to be augmented or replaced with several different types of genetic therapy to address the various problematic ion channels.
-
As previously noted, the HCN isoforms (e.g., HCN2 by itself instead of coupled to HCN4 in a functional heteromer) have different activation kinetics that consequently result in different HR ranges. Therefore, to simulate the complex SA node and its complex current, a variety of transfected genes may be required in a gene or cell therapy aimed at pacing dysfunction. Such a variety of genes can be obtained by using any one of the four different HCN isoforms, combinations of HCN isoforms in the form of heteromers or as multiple independent isoforms, or combinations of an HCN isoform or heteromer with other genes that affect heart rate. The heteromerization of the isoforms changes pacemaker electrophysiology via altered activation kinetics (e.g., allows for modulation (increase or decrease) of heart rate). Much B et al. J of Biol Chem; 44 (31): 43781-43786. While the exact stoichiometry of the heteromerized HCN channels has not been described yet, it is considered that these channels may form heteromers with a 3:1 ratio, but ratios of 1:1 or 1:3 are also possible as the HCN channels are known to form tetramers. In related rod photoreceptor cyclic nucleotide-gated channels, an asymmetrical stoichiometry of the two subunits present in the tetramers of 3:1 was determined. See, Zhong H et al. Nature 2002; 420: 193-196; See also, Weitz D et al. Neuron 2002; 36: 881-889 and Zheng J et al. Neuron 2002; 36: 891-896.
-
HCN3, or subunits thereof, is delivered to the heart in order to induce a slow depolarizing diastolic pacemaker current in atrial, ventricular or conductive tissue. See SEQ ID NO: 3. While HCN3 has not previously been considered as a gene therapy for pacing dysfunction, HCN3 can be used in a biopacemaker because, in part, HCN3 has similar kinetics to HCN2 (which is found in the heart). In fact, the homology between the two genes is approximately 86%. More importantly, the small current that is associated with HCN3 is significant in allowing for precise manipulation of biopacemaker current. Much et al., Role of Subunit Heteromerization and N-Linked Glycosylation in the Formation of Functional Hyperpolarization-activated Cyclic Nucleotide-Gated Channels, J. Biol. Chem. (2003) 278: 43781-43786. Furthermore, HCN3 is smaller in size than HCN1, HCN2 or HCN4. Consequently, it fits easily in a viral vector with limited “transgene carrying capacity” such as AAV. In addition, overexpression of HCN3 can strengthen the small current normally associated with the gene. Also, because HCN3 is not naturally present in the heart, but rather in the brain, a successful transfection of the gene into cardiac tissue is more readily identifiable than channels induced by, for example, HCN2, which are commonplace in cardiac tissue.
-
Various combinations of HCN genes (e.g., HCN3 and HCN4) may be delivered to the heart in order to induce a pacemaker current. See SEQ ID NOS: 1, 2 and 4. The HCN genes may work independently of one another or as functional heteromers. Different heteromers result in different voltage activation thresholds and channel kinetics that in turn result in different heart rate capacities. Other characteristic changes occur in the resultant AP associated with the transfected tissue. For example, certain HCN isoforms, such as HCN1, are not very responsive to cAMP whereas combining isoforms may result in a heteromeric channel which is more sensitive to cAMP.
-
Regarding heteromer formation, only one pair of channel subunits, HCN2 and HCN3, do not form a functional heteromer. HCN3 is resistant to forming heteromers. Therefore, as a consequence, expression is more predictable. Coexpression of HCN2 and HCN3 produces a current density less than that of cells that only express HCN2. The following combinations may all be used to vary the resultant current density: HCN1/HCN2, HCN1/HCN3, HCN1/HCN4, HCN2/HCN3, HCN2/HCN4 and HCN3/HCN4. When no heteromer is created, co-expression of two HCN genes still produces current levels that may be needed to obtain a desired pacemaker current. Coexpression of three or more subunits allows for further still more complicated channels with varying resultant pacemaker currents.
-
In mammalian hearts, different isoforms of HCN are being expressed. See review in Trends Cardiovasc Med. 2002 July; 12(5):206-12. For example, HCN2 is considered to be the primary isoform in atria and ventricles, while HCN4 is predominantly expressed in sinoatrial and atrioventricular nodal cells. Therefore, by administering an exogenous HCN isoform via gene therapy, it is very likely that heterodimer formation does occur in vivo. To proof this, we studied hyperpolarization activated (If) current in HL-5 cells, a cardiac cell line. See FIGS. 12 and 13. This cell line is a clone from HL-1 cells. In these cells, HCN expression has been shown, with the strongest signals for HCN2 mRNA, followed by HCN1 and little HCN3, and no HCN4. See, Journal of Physiology. 2002 545(1):81-92. Expression of HCN4 clearly changes the activation kinetics of If. See e.g., FIG. 12. The activation kinetics of endogenous HCN channels is distinct from HL-5 cells expressing HCN4-truncated. The resulting activation kinetics is also distinct from truncated HCN4 expressing HEK 293 cells. This suggests that heterodimer formation occurs also in vivo. This could be exploited therapeutically, for example by choosing different isoforms based on the specific delivery site (e.g. Purkinje system, AVN may require a different isoform than right atrial septum)
-
HCN genes or various combinations of HCN genes may also be combined with other genes and delivered to the heart in order to induce a pacemaker current. In addition, the non-HCN genes may be supplied independently of HCN genes. The non-HCN genes may, for example, increase the expression of a particular ion channel or suppress, in whole or in part, the expression of function of an ion channel. Such non-HCN genes can be made by traditional PCR-based amplification and known cloning techniques. Alternatively, such a gene or polynucleotide can be made by automated procedures that are well known in the art. Such a polynucleotide should include a start codon to initiate transcription and a stop codon to terminate translation.
-
One example of such a non-HCN gene encodes beta-adrenergic receptors (e.g., types 1 and 2) that increase HR when exposed to circulating catecholamines or norepinephrine that is released from sympathetic neurons. See SEQ ID NOS: 5-6.
-
Another example involves DNA that will suppress the KCNJ2 gene encoding for the inward potassium rectifier channel 2.1 (Kir2.1) that regulates Ik1 current. See SEQ ID NO: 10. Voltage-gated potassium (KV) channels represent the most complex class of voltage-gated ion channels from both functional and structural standpoints. Their diverse functions include regulating neurotransmitter release, heart rate, insulin secretion, neuronal excitability, epithelial electrolyte transport, smooth muscle contraction, and cell volume. This gene encodes a member of the potassium channel, voltage-gated, isk-related subfamily. This member is a small integral membrane subunit that assembles with the KCNJ2 gene product, a pore-forming protein, to alter its function. This gene is expressed in the heart and its mutations are associated with cardiac arrhythmia.
-
The import of using this gene is expression of HCN in the ventricle leads to an unstable cycle length in silico. If Ik1 expression is decreased by about 50%, however, a stable cycle length (heart rate) is seen. See, FIG. 6. Moreover, if expression of IK1 is further decreased to levels at or below 20%, then automaticity occurs in normal ventricular or atrial myocytes. This latter approach is described in detail in concurrently filed U.S. patent application claiming priority to U.S. Pat. App. Ser. No. 60/532,764. By combining the suppression of Ik1 with HCN expression, risks of action potential prolongation, increased dispersion of repolarization, ventricular tachycardia or fibrillation. and arrhythmogenesis may be further avoided. Therefore, a combination approach expression of HCN and suppression of IK1 is beneficial.
-
Other regulatory proteins include muscarinic (M2) and/or (M3) receptors for enhanced parasympathetic control that can result in a decreased HR. See SEQ ID NOS: 11-12. Muscarinic receptors influence many effects of acetylcholine in the central and peripheral nervous system. The muscarinic cholinergic receptor 2 is involved in mediation of bradycardia and a decrease in cardiac contractility. The muscarinic cholinergic receptors belong to a larger family of G protein-coupled receptors. A typical control signal mediated via the vagus nerve leads to a local release of acetylcholine (Ach) in the sinoatrial and atrioventricular nodes. Ach then binds to the M2 receptor, activates an inhibitory G protein (G.alpha.i), and essentially decreases the activity of adenylate cyclase, which directly leads to opening of K+ channels. In the sinoatrial node, vagal stimulation tends to flatten the diastolic depolarization, which then induces a slowing of heart rate (bradycardia, negative chronotropic effect), not only via the effects of reduced cAMP availability on if current (hyperpolarization activated cyclic nucleotide-gated channel), but also via activation of a potassium outward current. In the atrioventricular nodal tissue, vagal stimulation also activates an inhibitor G protein, which causes a slowing conduction velocity via a decreased calcium influx through L-type calcium channels. Clinically, the effects of vagal stimulation on the atrioventricular node are detected as increased atrioventricular nodal conduction times (e.g., prolonged PR interval).
-
In addition, the cells of the conduction system are genetically modified to increase the inward Ca2+ current by delivering a bio-pacemaker composition to these cells. As a specific example, for the Purkinje fibers, the composition includes a coding sequence that encodes a T-type Ca2+ channel resulting in the exogenous expression of T-type Ca2+ channels. More specifically, as an example, genes that promote T-type calcium channel overexpression (e.g., CaV3.1) are another example of this additional gene. Alpha-1 subunits of Ca(2+) channels, such as CACNA1H, consist of 4 homologous repeat domains. Each domain has six transmembrane segments, a highly conserved pore loop, and a distinctive voltage sensor. The voltage dependence and fast inactivation of CACNA1H results in transient, or T-type, electrical currents. See SEQ ID NOS: 7-8. Exogenous expression of this channel will facilitate the depolarization characteristics of, for example, Purkinje fiber cells necessary to increase their intrinsic pacing rate.
-
Another suitable polynucleotide encodes human voltage-gated channel (KCND3). See SEQ ID NO: 14. This is one of the subunits responsible for Ito (transient outward current). It is beneficial to suppress this gene (e.g., via siRNA, via dominant negative approaches, via ribozyme) to prolong action potential durations thereby mimicking the electrophysiology of SA nodal cells.
-
Yet another gene is the Human KV channel interacting protein 2, SEQ ID NO: 15. This presents another option for modulating Ito by suppressing this protein.
-
Non-human protein examples include, but are not limited to, Rabbit minK-related peptide, SEQ ID NO: 9, and HCN1, SEQ ID NO: 24, Rat HCN1-HCN4, SEQ ID NOS: 16-19, Mouse HCN1-HCN4, SEQ ID NOS: 20-23 and Rainbow Trout HCN1, SEQ ID NO: 25.
-
Other suitable polynucleotides useful in connection with the invention can be obtained from a variety of sources including, without limitation, GenBank (National Center for Biotechnology Information (NCBI)), EMBL data library, SWISS-PROT (University of Geneva, Switzerland), the PIR-International database; the American Type Culture Collection (ATCC) (10801 University Boulevard, Manassas, Va. 20110-2209); National Center of Biotechnology Information (https://www.ncbi.nlm.nih.gov/) and PubMed (https://www.ncbi.nim.nih.gov/entrez/query.fcgi?db=PubMed), both associated with the National Library of Medicine and National Institute of Health; PubMed.
Controlling the Selected Gene Construct
-
For site-specific expression of the transgene, tissue-specific promoters are made a part of the expression system. This tissue-specific expression significantly enhances the safety of the gene therapy as expression in non-target tissue becomes very unlikely.
-
For example, cardiac tissue specific promoters allow cardiac myocyte specific expression of the transgene of interest (including expression in stem cells with cardiac phenotype). As an example of one such promoter, a myosin heavy chain or myosin light chain promoter could be part of the expression system allowing transgene (e.g., HCN4) expression only in tissue containing this promoter (i.e., cardiac myocytes). Other examples of cardiac tissue specific promoters include, as examples, cardiac ankyrin repeat protein (U.S. Pat. No. 6,451,594), alpha-myosin heavy chain gene, beta-myosin heavy chain gene, myosin light chain 2 v gene a myosin light chain enhancer followed by either a myosin-heavy chain promoter or a viral promoter and a polynucleotide sequence (U.S. Published Patent Application 2002/025577 A1), myosin light chain 2a gene, cardiac alpha-actin gene, cardiac M2 muscarinic acetylcholine gene, ANF (ANP) atrial natriuretic factor (or peptide), cardiac troponin C, cardiac troponin I, cardiac troponin T or cardiac sarcoplasmic reticulum Ca-ATPase gene.
-
Specific promoters for the conductive system could also be employed if the site of the biological pacemaker is targeted at the cardiac conduction system. As an example, constructs of the present invention can be targeted to cells of the Purkinje network by methods known to those skilled in the art. Advantage can be taken of the expression of cell surface receptors unique to specific cells. For instance, one such receptor, preferentially expressed on the surface of Purkinje cells, is the cysteinyl leukotriene 2 receptor (CysLT2). This receptor distinguishes Purkinje cells from neighboring cells such as ventricular cells and can be utilized to target constructs of the invention preferentially to Purkinje cells. In the practice of the present invention, however, any receptor specific to Purkinje cells may be utilized for specific targeting.
-
Targeted delivery requires the modification of the vehicle delivering the construct (which will be more fully developed below). Several methods for modification of such vehicles are possible. For example, viral protein capsids or proteins of the viral envelope may be biotinylated for subsequent coupling to a biotinylated antibody directed against a specific receptor or ligand via a strepavidin bridge.
-
Alternatively, the viral delivery vehicle may be genetically modified so that it expresses a protein ligand for a specific receptor. The gene for the ligand is introduced within the coding sequence of a viral surface protein by, for example, insertional mutagenesis, such that a fusion protein including the ligand is expressed on the surface of the virus. For details on this technique see Han et al., “Ligand-Directed Retroviral Targeting of Human Breast Cancer Cells,” Proc. Natl. Acad. Sci., 92:9747-9751 (1995). Viral delivery vehicles may also be genetically modified to express fusion proteins displaying, at a minimum, the antigen-binding site of an antibody directed against the target receptor. See e.g., Jiang et al., “Cell-Type-Specific Gene Transfer into Human Cells with Retroviral Vectors That Display Single-Chain Antibodies,” J. Virol., 72: 10148-10156 (1998).
-
An embodiment of the invention may also involve regulation of the transgene via regulatory elements such as drug-sensitive elements (e.g., a drug-inducible suppressor or promoter). Drug-responsive promoters may induce or suppress gene expression. For example, a tetracycline responsive element (TRE) that binds doxycycline is present within the promoter construct. When doxycycline is removed, transcripton from the TRE is turned off in a highly dose-dependent manner. Examples of inducible drug-responsive promoters are the ecdysone-inducible promoter (U.S. Pat. No. 6,214,620) and rapamycin-dependent expression (U.S. Pat. No. 6,506,379). See Discher et al., J. Biol. Chem. (1998) 273:26087-26093; Prentice et al., Cardiovascular Res. (1997) 35: 567-576.
-
Other promoters, for example, would be sensitive to electrical stimulus that could be provided from, for example, an implantable device. Electrical stimulation can promote gene expression (U.S. Patent Application No. 2003/0204206 A1). This would allow for turning automaticity of the cells on and off, or modulating there between.
Delivering the Selected Gene Construct
-
The gene construct may be transfected into target cells such as endogenous cardiac cells (e.g., myocytes), stem cells, myoblasts or other cells. Endogenous cells such as atrial or ventricular cells or cells of the conduction system are transfected using local delivery of a genetic therapy via catheter, direct injection, or equivalent delivery means. Other cells may be transfected outside of the body and then delivered to the heart using a catheter or equivalent means. For example, as will be appreciated by those skilled in the art, cardiac myocardial cells derived from stem cells may be treated with the genetic procedures described herein and implanted into a region of the conduction system (e.g. Purkinje fiber) with a catheter or by direct injection to Purkinje fiber tissue.
-
The genetic construct can be delivered into a cell by, for example, transfection or transduction procedures. Transfection and transduction refer to the acquisition by a cell of new genetic material by incorporation of added nucleic acid molecules. Transfection can occur by physical or chemical methods. Many transfection techniques are known to those of ordinary skill in the art including, without limitation, calcium phosphate DNA co-precipitation, DEAE-dextrin DNA transfection, electroporation, naked plasmid adsorption, and cationic liposome-mediated transfection. Transduction refers to the process of transferring nucleic acid into a cell using a DNA or RNA virus. Suitable viral vectors for use as transducing agents include, but are not limited to, retroviral vectors, adeno associated viral vectors, vaccinia viruses, adenoviral viruses, epstein barr viruses, coxsackie viruses and sendai viruses.
-
The selection of a delivery means at the cellular level should address the length of desired expression. For example, where permanent pacing therapy is desired, an adeno-associated virus (AAV) encoding HCN4 and an additional AAV encoding regulatory receptor proteins, such as beta-adrenergic or muscarinic receptors, is implemented. AAVs have good long-term expression qualities because of their ability to integrate their genome into non-dividing cells in addition to their minimal immune response.
-
AAV vectors can be constructed using techniques well known in the art. Typically, the vector is constructed so as to provide operatively linked components of control elements. For example, a typical vector includes a transcriptional initiation region, a nucleotide sequence of the protein to be expressed, and a transcriptional termination region. Often, such an operatively linked construct will be flanked at its 5′ and 3′ regions with AAV ITR sequences, which are required viral cis elements. The control sequences can often be provided from promoters derived from viruses such as, polyoma, Adenovirus 2, cytomegalovirus, and Simian Virus 40. Viral regulatory sequences can be chosen to achieve a high level of expression in a variety of cells. Alternatively, ubiquitous expression promoters, such as the early cytomegalovirus promoter can be utilized to accomplish expression in any cell type. A third alternative is the use of promoters that drive tissue specific expression (addressed above). This approach is particularly useful where expression of the desired protein in non-target tissue may have deleterious effects. Thus, according to another preferred embodiment, the vector contains the proximal human brain natriuretic brain (hBNP) promoter that functions as a cardiac-specific promoter. For details on construction of such a vector. See, LaPointe et al., “Left Ventricular Targeting of Reporter Gene Expression In Vivo by Human BNP Promoter in an Adenoviral Vector,” Am. J. Physiol. Heart Circ. Physiol., 283:H1439-45 (2002).
-
Vectors may also contain cardiac enhancers to increase the expression of the transgene in the targeted regions of the cardiac conduction system. Such enhancer elements may include the cardiac specific enhancer elements derived from Csx/Nkx2.5 regulatory regions disclosed in the published U.S. Patent Application 2002/0022259.
-
The subject invention may utilize an adeno-associated virus (AAV) but could also use a 2nd or 3rd generation adenovirus or others such as chimeric adeno-associated virus (AAV1/2) which is the chimeric product of AAV1 and AAV2 vectors. The AAV1 and AAV2 serotypes differ in composition of their capsid protein coat with resultant varying characteristics. The AAV2, for example, can be beneficial due to its known receptor binding and known approach for purification. AAV 1 allows for good muscle transfection. Cross-packaging of a single AAV type 2 vector genome into multiple AAV serotypes enables transduction with broad specificity. AAV 1/2 combines the advantages of these two vectors regarding, for example, purification and muscle transfection. FIG. 10 depicts an image of truncated HCN as expressed in cells that were transduced with constructs containing AAV1/2.
-
In one example of the invention, human HCN3 gene, SEQ ID NO: 3, can be cloned into a chimeric adeno-associated virus (AAV1/2) with the following sequence: AAV-CAG-humanHCN3-WPRE-BGHpolyA. A control vector encoding GFP is an adeno-associated virus (AAV1/2) with the following sequence: AAV-CAG-eGFP-WPRE-BGHpolyA. A CAG promoter (hybrid chicken B-actin/CMV enhancer) is used to achieve high transgene expression. Also, as a post-regulatory element, woodchuck postregulatory regulatory element (WPRE) can be used thereby allowing for increased transgene expression levels. Other common vectors are provided in U.S. Pat. Application No. US 2002/0155101A1. Suitable vectors can be obtained at GeneDetect.Com, 1455 Tallevast Road, Suite L8299, Sarasota, Fla. 34243 as well as other organizations known in the art.
-
When selecting a vector, using an AAV for example, a problem can arise if the HCN transgene does not fit into common AAV expression cassettes. Such problems are amplified when promoters and additional regulatory elements are included in the cassette. See, FIGS. 3 and 4. For example, when using GeneDetect's rAVE cassette, this problem is overcome with HCN3 (2,334 base pairs (“bp”) by removing a regulatory element (e.g., SAR) from the cassette. For HCN2 (2,670 bp), an additional element (e.g., WPRE) can be left out. For large genes such as HCN4 (3,612 bp), however, the transgene size must be further reduced by truncating the very large C-terminus. In one embodiment, truncation of the sequence occurs not before the cAMP binding site which still allows for a functional gene. For example, with HCN2, by 2161-2670 may be truncated. Bp 1654-2010 is the cAMP binding site. As another example, with HCN3 bp 1813-2325 may be truncated. Bp 1306-1662 is the cAMP binding site. As an additional example, as depicted in FIG. 8, HCN4 may be truncated from base pair 3612 to base pair 2313. Here, base pairs 1807-2163 represent the cAMP binding site. As an additional example, with HCN1 the C-terminus, including the cAMP binding site, may also be truncated as this protein isoform demonstrates very little responsiveness to cAMP binding.
-
At the macro level (i.e., non-cellular level), various catheter means may be employed to deliver the gene construct to the heart tissue. FIG. 2 shows a guide catheter 90 being positioned for delivery of the genetic construct of the invention. A venous access site (not shown) for the catheter 90 may be in a cephalic or subclavian vein. Means used for venous access are well known in the art and include the Seldinger technique performed with a standard percutaneous introducer kit. The guide catheter 90 includes a lumen (not shown) extending from a proximal end (not shown) to a distal end 92 that slideably receives the delivery system 80. The guide catheter 90 may have an outer diameter between approximately 0.115 inches and 0.170 inches and be of a construction well known in the art. The distal end 92 of the guide catheter 90 may include an electrode (not shown) for mapping electrical activity in order to direct the distal end 92 to an implant site near certain pacing areas in the heart. Alternatively, a separate mapping catheter may be used within the lumen of the guide catheter 90 to direct the distal end 92 to an application site near certain areas of the heart. This method is well known in the art. Other catheter means are described in commonly-assigned co-pending U.S. patent application Ser. No. 10/262,046, filed Oct. 2, 2002; and Ser. No. 10/423,116, filed Apr. 23, 2003, both of which are incorporated herein by reference.
-
In short, delivery of a genetic construct can be carried out according to any method known in the art (e.g., syringe injection). It is only necessary that the genetic construct reach a small portion of the cells that are targeted for gene manipulation (e.g. cells of the Purkinje fibers). The genetic construct may be injected directly into the myocardium as described by R. J. Guzman et al., Circ. Res., 73:1202-1207 (1993). The delivery step may further include increasing microvascular permeability using routine procedures, including delivering at least one permeability agent prior to or during delivery of the genetic construct. Perfusion protocols useful with the methods of the invention are generally sufficient to deliver the genetic construct to at least about 10% of cardiac myocytes in the mammal. Methods for targeting non-viral vector genetic constructs to solid organs, for example, the heart, have been developed such as those described in U.S. Pat. No. 6,376,471. Additional non-injection methods for gene delivery include, but are not limited to, polymer-based gene-delivery (e.g. via coated devices, via biodegradable scaffolds), gene delivery via cells attached to a device or to a biodegradable scaffold, gene delivery via vascular or transvascular delivery into selected myocardial regions, gene delivery via aid of electroporation or gene delivery via other means.
-
As an example of solution concentrations and dosage levels, concentrations of 1×107 to 1×1013 parts gene construct per 100 microliters of solution of phosphate buffered saline may be used in dosages of 20-200 microliters. Also, 1:1 concentrations of different HCN isoforms and other genes may be used (e.g., HCN4 and genes encoding beta-adrenergic receptors). Still, other concentrations and dosage levels will be apparent to those skilled in the art as the effective dose of the gene construct will be a function of the particular expressed gene(s), the particular cardiac arrhythmia to be targeted, the desired heart rate (e.g., 60-90 beats per minute at rest and appropriate modulation of heart rate during stress or exercise as well as during sleep), the patient and his or her clinical condition, weight, age and sex. Other examples include administering several dosages in several locations. For example, a primary biological pacemaker in the atrial septum may be utilized, and in case of AVN conduction block, a backup pacemaker (with a lower intrinsic rate) in the ventricle (e.g. myocardial cells of Purkinje system).
Verification of Enhanced Pacemaker Current
-
Methods for detecting modulation of the cells of the conduction system of the heart by electrophysiological assay methods relates to any conventional test used to determine the cardiac action potential characteristics, such as action potential duration (APD). Briefly, a standard electrophysiological assay includes the following steps: providing a mammalian heart (in vivo or ex vivo), delivering to the heart a genetic construct or modified cells of the invention, transferring the genetic construct and/or modified cells into the heart under conditions which can allow expression of an encoded amino acid sequence, and detecting the increase of electrical properties in the cells of the heart to which the genetic construct and/or modified cells were delivered, wherein at least one property is the pacing rate of the cells, relative to a baseline value. Baseline values will vary with respect to the particular target region chosen in the conduction system.
-
Additionally, modulation of cardiac electrical properties obtained with the methods of the invention may be observed by performing a conventional electrocardiogram (ECG) before and after administration of the genetic construct of the invention and inspecting the ECG results. ECG patterns from a heart's electrical excitation have been well studied. Various methods are known for analyzing ECG records to measure changes in the electrical potential in the heart associated with the spread of depolarization and repolarization through the heart muscle. A preferred method of monitoring the proper function of a biological pacemaker may be via an implantable pacemaker/defibrillator or an implantable loop-recorder (e.g. Medtronic's Reveal™). Other methods include placement of endocardial mapping electrode catheters to various locations in the heart, and record an intrinsic local electrical signal (EGM). These procedures require venous or arterial access to the endocardium of the atrial or ventricular tissue. These mapping catheters can be used in conjunction with analog or digital systems which range from simple electrophysiological assessments (e.g. GE Prucka system) to more complex electroanatomical maps of the heart (e.g. Carto or Endocardial Solutions systems). Such mapping procedures are well known in the art.
-
For whole-cell voltage-clamp experiments, using the following as an example, experiments may be conducted at room temperature using traditional instrumentation known in the art such as, but without limitation, an Axon Instruments 200A amplifier and Nikon Inverted Microscope (100T). Borosilicate glass microelectrodes (1-3 Megaohms) can be sealed to the lipid bilayer membrane of cells and the transmembrane currents at various holding potentials can be measured via a small rupture within the seal. The cells can be bathed in an extracellular-like solution that may include, but is not limited to, the following reagents and concentrations (in millimolar): NaCl (110), MgCl2 (0.5), KCl (30), CaCl2 (1.8), Hepes (5), and pH=7.4 (w/NaOH). Likewise, the microelectrode inner lumen may contain, but is not limited to, the following reagents and concentrations (in millimolar): NaCl (10), MgCl2 (0.5), KCl (130), EGTA (1), Hepes (5), and pH=7.4 (w/KOH).
-
The voltage clamp protocol involves a holding potential of −40 mV (1 second) and then conducting sweeps (3 second duration) in −10 mV steps from −40 mV to −140 mV. The last step of the protocol is either holding it at −40 mV or at −140 mV for 1 second.
-
FIG. 5 shows one example of the aforementioned patch clamp experimentation. The recordings were obtained from whole-cell patch clamp experiments using human embryonic kidney 293 (HEK 293) cells that were co-transfected with an adeno-associated virus encoding enhanced green fluorescent protein (AAV1/2-CAG-eGFP) and an adeno-associated virus encoding the human HCN3 gene (AAV1/2-CAG-HCN3). When the cells were hyperpolarized to −140 mV, a slowly activating inward current was detected that was characteristic of HCN channels. No inward current was detected in control cells (not transfected cells) or cells transfected only with AAV-eGFP when the voltage was held at −140 mV (data not shown).
-
FIG. 7 depicts a fluorescence microscopic image demonstrating positive GFP expression four weeks after injection of rAAV-eGFP into canine myocardium.
Example I
-
HL-5 cells at passage 73 were cultured in gelatin-fibronectin coated 33 mm culture dishes. Cells were maintained in the medium (JRH Biosciences, Lenexa, Kans., USA), supplemented with 10% fetal bovine serum, 4 mM L-glutamine, 10 .mu.M noradrenaline (norepinephrine; Sigma Aldrich, St. Louis, USA) and penicillin-streptomycin. The medium was changed every 24 h. HL-5 cells at different passages (from 75 to 98) were splitted when they reached a state of confluence. Dissociated cells were either re-plated for a new passage or used for patch clamp experiments. Some cells were transfected with rAAV-HCN4tr-cmyc. Cells were cultured at 37° C. under an atmosphere of 5% CO2 and 95% air with approximately 95% humidity.
-
After dissociation from a culture dish, cells were plated on gelatin/fibronectin-coated coverslips for patch-lamp experiments. During an experiment HL-5 cells plated on a coverslip were transported to a chamber mounted on the stage of a Nikon microscope. The chamber was continuously superfused (1 ml/min) with the Tyrode's solution, which contained (in mM): 140 NaCl, 5.4 KCl, 1.8 CaCl2, 1 MgCl2, 10 HEPES, and 10 glucose (pH 7.4 adjusted with NaOH). The whole-cell configuration of the patch-clamp technique (Hamill et al. 1981) was applied in the experiments. Briefly, glass electrodes (World Precision Instruments, Sarasota, Fla.) with 2-4 M.OMEGA. resistance were connected via a Ag—AgCl wire to an Axopatch 200A amplifier interfaced with a DigiData 1320 acquisition system. After forming a conventional “gigaohm” seal, electrode capacitance was compensated. Whole-cell configuration was achieved by rupturing the membrane with additional suction. Membrane capacitance and series resistance were compensated to reduce artifactual distortion. A perfusion system (Warner Instruments, Inc., Hamden, Conn., USA) was used to change the extracellular solution. Data were collected with the pCLAMP software (version 9.2, Axon Instruments, Foster City, Calif.). Experiments were conducted at room temperature (23° C.).
-
Before electrical compensation, cell membrane capacitance (Cm) was measured in each patched cells with the pCLAMP program. During recordings, the cells were superfused with the modified Tyrode's solution to measure If. The bath solution contained (mM): NaCl 140; KCl 5.4; CaCl2 1.8; MgCl 2 1; D-glucose 10; Hepes 10 (pH adjusted to 7.4 with NaOH) and supplemented with (mM): NiCl 2; BaCl 2 2; CdCl 0.2; 4-aminopyridine 1 to eliminate Ca2+ current (T- and L-type), inward rectifier K+ current, IK1 and transient outward K+ current, It0, respectively. KCl was increased to 25 mM to amplify If. Pipette solution contained (mM): K-glutamate 130; KCl 15; NaCl 5; MgATP 5; MgCl 2 1; EGTA 5; CaCl 2 1; Hepes 10 (pH adjusted to 7.2 with KOH). If currents were evoked by 2 to 6 s hyperpolarizing steps to potentials ranging from −50 to −130 mV from a holding potential of −40 mV. A single-exponential fit of the current traces evoked at different potentials allowed derivation of time constants (.tau.) of current activation. The initial delay of the current was excluded from the fitting.
-
The reversal potential of If was evaluated by tail currents recorded by 1.2 s ‘tail’ steps to membrane potentials ranging from −80 to 0 mV in 10 mV step intervals followed a 2 s conditioning potential step to −120 mV. The holding potential was set at −40 mV. The amplitudes of tail currents were then plotted against the test potentials. The current-voltage (1-V) relationship was fitted with a linear regression equation and the intersection on the x-axis was the reversal potential of I. The activation of If was calculated by tail currents elicited by 3 s ‘tail’ pulses to −120 mV followed 5 s conditioning pulses from −130 mV to −60 mV in 10 mV increments every 10 s. The holding potential was −40 mV. The amplitudes of tail currents were then normalized to the maximal current and plotted against the conditional pulses. Activation data were fitted by a Boltzmann function.
-
As shown in FIG. 12, current traces of If recorded from HL-5 cells. A, the voltage-clamp protocol. B, superimposed If traces were recorded from a non-transfected HL-5 cell. C, superimposed If traces were recorded from a HCN4-transfected HL-5 cell. D, current-voltage relationships of If were plotted according to the values measured at the places of the vertical dotted lines for the control (∘) and HCN4-transfected () HL-5 cells. Test pulses from −50 mV to −130 mV in 10 mV increments were applied. The holding potential was −40 mV and stimulation rate was 0.2 Hz. The arrows in panel A and B indicate the zero current level. The dotted horizontal line in panel D indicates the zero current level.
-
FIG. 13 provides a comparison of activation kinetics of If recorded in control and HCN4-transfected HL-5 cells (using rAAV-HCN4tr-cmyc). Superimposed current traces were elicited by test pulses (see the insets) from −40 mV to −120 mV (A) and from −40 mV to −130 mV (B) for the control (black trace) and HCN4-transfected (red trace) HL-5 cells. The maximal currents recorded from the control cell were normalized (by 5.4-fold for −120 mV and 5.1-fold for −130 mV) close to the maximal current of the HCN4-transfected cell. Time constants (.tau.) of activation of If were fitted with the equation of single exponential decay.
Example II
hHCN4-Channel Truncated Versus Full-Length hHCN4 Channel
-
Experiments were carried out to characterize the hHCN4-channel truncated 16 amino acids after the end of the cyclic nucleotide binding domain (CNBD). The truncated hHCN4 was compared to the full-length hHCN4 channel. See e.g., SEQ ID NOS. 4, 28 and 29. Electrophysiological experiments were carried out as described in Ludwig A., Zong X., Stieber J., Hullin R., Hofmann F. and Biel M., Two Pacemaker Channels From Human Heart With Profoundly Different Activation Kinetics, EMBO J. 1999, 19 (9):2323-2329 and Stieber J., Thomer A., Much B., Schneider A., Biel M. and Hofmann F., Molecular Basis For The Different Activation Kinetics of The Pacemaker Channels HCN2 and HCN4, J Biol Chem 2003, 278 (36):33672-33680.
-
Using the FuGENE6 transfection reagent (Roche), HEK 293 cells were transiently transfected with one of the following cDNA constructs: (1) hHCN4 in the expression vector pcDNA3; (2) hHCN4 in the expression vector pIRES2-EGFP (bicistronic); (3) hHCN4, truncated 16 amino acids after the end of the CNBD, in the expression vector pcDNA3; or (4) hHCN4, truncated 16 amino acids after the end of the CNBD, in the expression vector pIRES2-EGFP (bicistronic).
-
HEK 293-cells were cultured in Quantum 286 complete medium (PAA Laboratories) on polylysated glass coverslips and kept at 37° C., 6% CO2 until ready to use. Two to three days after transfection currents were recorded in the whole cell recording technique at a temperature of 22±1° C.
-
The bath solution contained the following constituents in mM: 120 NaCl, 20 KCl, 1 MgCl2, 1.8 CaCl2, 10 HEPES, 10 Glucose, pH adjusted to 7.4 with NaOH. The pipette solution contained (in mM): 10 NaCl, 30 KCl, 90 K-Asp, 1 MgSO4, 5 EGTA, 10 HEPES, pH adjusted to 7.4 with KOH. Patch pipettes were pulled from borosilicate glass and had a resistance of 2-5 M.OMEGA. when filled with this pipette solution.
-
For determination of the effect of cAMP on the channels, 100 .mu.M 8-Br-cAMP (Sigma) was added to the bath solution. Data were acquired using an Axopatch 200B amplifier and pClamp7-software (Axon Instruments) and low-pass filtered at 2 kHz with an 8-pole Bessel filter (LPBF-48DG, npi). Data were evaluated using the Origin 6.0 software (Microcal). All values are provided as mean±SEM (standard error of the mean); 11-19 measurements (n) were evaluated per channel. Statistical differences were determined using Student's unpaired t-test; p-values<0.05 were considered significant.
-
To characterize the basic properties of the channels, the following was determined: (1) voltage-dependent activation curves with half-maximal activation (V1/2); (2) voltage dependence of activation time constants T (activation kinetics) (both in the presence and absence of 100 .mu.M cAMP); and (3) current—voltage relation with reversal potential (Erev).
-
To determine activation curves and activation kinetics, a pulse protocol was used as shown in FIG. 18 where the holding potential was −40 mV and 10 mV-step pulses of 5 seconds duration from −140 mV to −30 mV, followed by a step to −140 mV for 2 seconds; 30 seconds between consecutive activation steps.
-
With the protocol shown in FIG. 18, example current recordings were obtained from the truncated hHCN4 in pIRES2-EGFP and are shown in FIG. 19.
-
Time constants of activation (Tact) were obtained by fitting the current traces of the −140 to −90 mV steps after the initial lag with the sum of two exponential functions
-
y=A 1 e (x/τ1) +A 2 e (−x/τ2),
-
where T1 and T2 are the fast and slow time constants of activation, respectively; T1 is consequently referred to as Tact since A1 accounts for most of the current amplitude.
-
To obtain voltage-dependent steady-state activation curves, tail currents measured immediately after the final step to −140 mV were normalized by the maximal current (Imax) and plotted as a function of the preceding membrane potential. The curves were fitted with the Boltzmann function:
-
(I−I min)/(I man −I min)=(A 1 −A 2)/(1+e (V−V1/2K))+A 2,
-
where Imin is an offset caused by a nonzero holding current and is not included in the current amplitude, V is the test potential, V1/2 is the membrane potential for half-maximal activation, and K is the slope factor.
-
To determine reversal potential, a pulse protocol was used as shown in FIG. 20 where the holding potential was −40 mV, the full activation of the channels held at −140 mV for 8 seconds, and 10 mV-step pulses to −100 mV to +40 mV and 30 seconds between consecutive activation steps.
-
With the protocol shown in FIG. 20, example current recording was obtained from the truncated hHCN4 in pIRES2-EGFP and is shown in FIG. 21.
-
To determine the reversal potential, the tail currents obtained immediately after the step to the test voltages were plotted against the voltage. Thus, E, is the potential where the current is 0.
-
The voltage-dependent activation results are shown in FIG. 22. Generally, the truncated hHCN4-channel (“hHCN4trunc”, black circles) is voltage-dependently activated like the full-length hHCN4 (“hHCN4”, blue squares). V1/2 (half-maximal activation or midpoint of activation) does not differ significantly between hHCN4 and hHCN4trunc, being about −96 mV for both. In addition, both channels are modulated by cAMP (open symbols) to the same extent, i.e. 100 .mu.M cAMP induces a shift of the activation curve of −13 mV towards more positive activation potentials. However, the slope factor k differs significantly, both between the two unmodulated and between the two cAMP-modulated curves. Thus, the slope of the full-length hHCN4 is slightly steeper than that of the truncated channel, implying that the truncated channel may be activated over a broader range of potentials. This is particularly important for the present invention because it suggests that the truncated human HCN4 channel is more responsive to cAMP at physiological voltages, thereby making it a more desirable gene candidate for a biological pacemaker therapy.
-
The following table gives the key parameters of the voltage-dependent activation:
-
| |
| |
|
|
Significance |
| |
hHCN4, full length |
hHCN4, truncated |
of difference |
| |
n = 19 |
n = 17 |
(p-value) |
| |
| |
| V1/2 |
−96.7 mV |
−96.1 mV |
P > 0.5 |
| SD |
4.01 |
3.44 |
|
| SEM |
|
|
|
| Slope factor K |
11.0 |
14.3 |
P < 0.001 |
| SD |
1.15 |
2.45 |
|
| SEM |
0.31 |
0.71 |
|
| V1/2 |
−83.7 mV |
−83.2 mV |
P > 0.5 |
| SD |
6.22 |
3.73 |
|
| SEM |
2.54 |
1.18 |
|
| Slope factor K |
9.1 |
12.7 |
P < 0.001 |
| SD |
1.33 |
2.11 |
|
| SEM |
0.47 |
0.67 |
|
| Shift induced by 100 μM 8-Br-cAMP: |
-
Time constants of activation Tact at activation voltages from −140 mV to −90 mV (note logarithmic scale of y-axis) are shown in FIG. 23. Both channels are modulated by cAMP, i.e., the time constants of activation over the whole range of potentials measured are shifted to smaller values. Therefore, the channels are 2- to 3-fold faster activated in the presence of cAMP. Comparing Tact for each activation potential reveals that at potentials positive to −120 mV, the truncated hHCN4-channel tends to activate slightly faster than the full-length channel. This difference becomes significant only at −90 mV, both under nonmodulated and cAMP-modulated conditions.
-
As shown in FIG. 24, the reversal potential for both the full-length and truncated hHCN4 was determined in 20 mM extracellular potassium, without cAMP. It is −11.5 mV for hHCN4 and −16.2 mV for hHCN4trunc. The difference is not significant.
-
The human HCN4 channel, which is truncated 16 amino acids after the end of the cyclic nucleotide binding domain, can be well expressed in HEK 293-cells. The number of successfully transfected, i.e. HCN4-channel (current) and EGFP-(constructs in the pIRES2-EGFP-vector) expressing cells is approximately the same for all 4 tested constructs. Green-fluorescent cells can be well selected e.g. using excitation (filter) at .lamda.=450-490 nm and detection at A=505-530 nm).
-
Both the full-length and truncated constructs display similar, HCN4-like currents. The currents are of comparable amplitude and can be modulated by cAMP to the same extent. cAMP shifts the activation curve of both channels about 13 mV to more positive activation potentials and accelerates the activation about 2-3-fold (voltage dependent).
-
There is a slight but significant difference between the full-length and truncated hHCN4-channels. The slope of the voltage-dependent activation curve is steeper for the full-length channel. This could mean that the truncated hHCN4 channel can be activated over a broader range of membrane potentials even though this is not reflected in the value of the midpoint of activation V1/2 which is about −96 mV for both channels.
-
In addition to this difference in the voltage-dependent activation, there is a tendency for the truncated hHCN4-channel towards faster time constants of activation. This difference, however, is only significant at an activation potential of −90 mV.
-
All patents and publications referenced herein are hereby incorporated by reference. Referenced web sites are not incorporated by reference. It will be understood that certain of the above-described structures, functions and operations of the above-described preferred embodiments are not necessary to practice the present invention and are included in the description simply for completeness of an example embodiment or embodiments. In addition, it will be understood that specific structures, functions and operations set forth in the above-referenced patents and publications can be practiced in conjunction with the present invention, but they are not essential to its practice. It is therefore to be understood that within the scope of the claims, the invention may be practiced otherwise than as specifically described without actually departing from the spirit and scope of the present invention.