USRE37861E1 - Laryngoscope blade - Google Patents
Laryngoscope blade Download PDFInfo
- Publication number
- USRE37861E1 USRE37861E1 US09/654,222 US65422200A USRE37861E US RE37861 E1 USRE37861 E1 US RE37861E1 US 65422200 A US65422200 A US 65422200A US RE37861 E USRE37861 E US RE37861E
- Authority
- US
- United States
- Prior art keywords
- blade
- arcuate body
- proximal portion
- width
- laryngoscope
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Expired - Lifetime
Links
Images

Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B1/00—Instruments for performing medical examinations of the interior of cavities or tubes of the body by visual or photographical inspection, e.g. endoscopes; Illuminating arrangements therefor
- A61B1/267—Instruments for performing medical examinations of the interior of cavities or tubes of the body by visual or photographical inspection, e.g. endoscopes; Illuminating arrangements therefor for the respiratory tract, e.g. laryngoscopes, bronchoscopes
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B1/00—Instruments for performing medical examinations of the interior of cavities or tubes of the body by visual or photographical inspection, e.g. endoscopes; Illuminating arrangements therefor
- A61B1/06—Instruments for performing medical examinations of the interior of cavities or tubes of the body by visual or photographical inspection, e.g. endoscopes; Illuminating arrangements therefor with illuminating arrangements
Definitions
- the present invention relates to laryngoscopes, and particularly to an improved blade for a laryngoscope.
- a laryngoscope may be used to visually examine the larynx, its more important function is to aid endotracheal intubation.
- the need for intubation may arise during a controlled situation, such as surgery, or in a crisis situation when the patient is unable to breathe adequately and requires a resuscitation bag or mechanical ventilation.
- a flexible tube is inserted through the nasal or oral cavity, passed through the larynx, and into the trachea for the administration of gases.
- the larynx may be viewed as a chamber bounded superiorly by the epiglottis, inferiorly by the vocal cords which cover the opening to the trachea, anteriorly by the thyroid cartilage or Adam's apple, and posteriorly by a portion of the pharynx.
- the epiglottis is a lamella or leaf-like plate of cartilage which extends dorsally like a loose lid over the larynx, helping to protect the trachea by preventing food from entering the trachea during swallowing.
- the laryngoscope generally comprises a handle, a blade which is used to move the patient's tongue out of the way and to lift the epiglottis to expose the vocal cords, and a light source to illuminate the glottis and vocal cords.
- the two most widely used blades in the current state of the art are known as the Miller blade and the Macintosh blade.
- the Miller blade is a substantially straight blade with a curved tip, the curve commencing approximate 2 inches from the end of the blade.
- the Macintosh blade is a blade which is curved for substantially its entire length (U.S. Pat. No. 2,354,471 issued Jul. 25, 1944).
- the Miller blade is inserted along the longitudinal axis of the larynx past the epiglottis to lift it enough to visualize the vocal cords and slip the tube through the cords into the trachea.
- the Macintosh blade is inserted on a combination of the axis of the oral cavity and the longitudinal axis of the larynx, the tip being placed in the vallecula, which are shallow depressions in the membranous folds and tissue between the epiglottis and the root of the tongue. By applying an upward pressure at the vallecula, the epiglottis is raised enough to visualize the vocal cords.
- U.S. Pat. No. 5,036,835 issued Aug. 6, 1991 to Filli describes a blade which slides to adjust the length of the blade.
- U.S. Pat. No. 5,065,738 describes a sheath fitting over the blade to protect the patient's teeth, gums, oral mucosa and epiglottis from damage during insertion of the laryngoscope.
- the present invention exploits the principle used by health care providers to widen the airway in preparation of intubation.
- the airway is narrow. It is therefore recommended that the intubator align the laryngeal and pharyngeal axes; unlike the present invention, in this position neither the Miller blade nor the Macintosh blade present the optimum angle for viewing and intubating the patient.
- the Macintosh blade is curved, the curvature is greater than the curvature of the airway, hence it does not permit optimal visualization of the vocal cords because the intubator can't see around the curvature of the blade.
- the intubator has difficulty visualizing the tip of the blade, again due to the shape of the blade and the shape of the airway. Consequently the intubator has difficulty determining when the tip is in proper position.
- the present invention is a laryngoscope blade which is generally curved throughout its length. However, the curvature is more gradual than the curvature of the conventional Macintosh blade.
- the invention also provides the tip of the blade with a small reverse curve at the tip of the blade, in order to permit better visualization of the position of the end of the blade.
- the laryngoscope blade of the present invention further includes a proximal part which is contoured to the width and shape of the mouth, having a width of up to 6 cm., in order to provide better control of the tongue during laryngoscopy.
- This configuration is unlike the part of a conventional laryngoscope blade proximal to its connection with the handle, which is used to move the tongue away from the airway and prevent the tongue from obstructing visualization of the larynx. Therefore, present laryngoscope blades have a maximum width of approximately 2 cm.
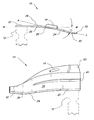
- FIG. 1 is a right side view of the improved laryngoscope blade according to the present invention.
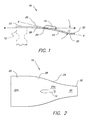
- FIG. 2 is a top plan view of the improved laryngoscope blade according to the present invention.
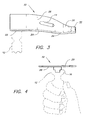
- FIG. 3 is a top perspective view of the improved laryngoscope blade according to the present invention.
- FIG. 4 is an end view of the improved laryngoscope blade according to the present invention.
- FIG. 5 is an environmental perspective view of an alternative embodiment of the invention showing a “bite block”.
- FIG. 6 is an end view of an alternative embodiment of the invention showing a “bite block” and raised areas on the surface of the blade defining grooves.
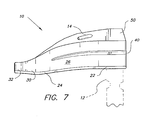
- FIG. 7 is a top perspective view of an embodiment of the invention with a vertical wall and a raised area defining grooves on the blade.
- a conventional laryngoscope typically comprises a handle, a blade, and a light source.
- the blade is usually pivotally mounted on the blade so that the blade is substantially parallel to the handle when not in use, and is substantially perpendicular to the handle to form an L-shape in use.
- a variety of arrangements may be used to provide a light source.
- Power for the light source is usually provided by batteries in the handle.
- the light source itself may be in the handle with a conduit mounted on the blade, or the light source itself may be mounted on the blade.
- the connector used to mount the blade may vary depending on the nature of the light source.
- the improvement of the present invention does not relate to the handle, the light source, or the means connecting the blade to the handle.
- the present invention relates to the laryngoscope blade 10 .
- the improved blade is designed to be used with a conventional handle 12 (shown in phantom in the drawings), means for illumination 14 , and means 16 for connecting the blade 10 to the handle 12 , all of which are well known in the prior art.
- the light source 14 is shown mounted on the top surface of the blade 10 in FIGS. 1 through 3, it will be appreciated that the light source 14 may be mounted alternatively on the edge of the blade 10 , or in the handle 12 with a light-transmitting conduit towards the end of the blade 10 , etc.
- the nature and location of the means for illumination 14 are not critical, provided that there are some means for illuminating the distal end of the blade 10 and an appropriate means 16 for connecting the blade 10 to the handle 12 adapted to the particular light source used.
- the improved blade 10 has an arcuate body 20 having a proximal end 22 and a distal end 24 , the body 20 being substantially flat, having a top surface 26 which is convex upwards as seen from a side view, and a bottom surface 28 concave downwards.
- the means 16 for connecting the blade 10 to the handle 12 is connected to the bottom surface 28 of the proximal end 22 of the body 20 .
- the blade 10 has a tip 30 at the distal end 24 of the body 20 , the tip 30 having a point of inflection as seen from a side view, most clearly seen in FIG. 1, and a short tip extension 32 being concave upwards.
- the tip extension 32 provides the physician or other person performing the intubation with a visual means for determining the depth to which the blade 10 has been inserted into the patient's throat, and can be rested on the top of the epiglottis, both features being an improvement on prior laryngoscope blades.
- the top surface 26 and the bottom surface 28 of the blade 10 have a proximal portion 22 a towards the proximal end 22 of the body 20 having a width of between 2 cm and 6 cm in the preferred embodiment, the proximal portion 22 a having a substantially oblong shape, so the that proximal portion 22 a conforms to the width of an adult patient's mouth.
- the top surface 26 and the bottom surface 28 have a distal portion 24 a towards the distal end 24 of the body 20 .
- the width of the blade 10 tapers from the proximal portion 22 a to a width not greater than approximately 2 cm at the distal end 24 , so that the distal end 24 may be inserted in the patient's throat.
- the blade 10 will be made in various sizes, with perhaps the width of the proximal portion of the body 20 ranging between 2 cm and 6 cm in 0.5 cm increments, while the distal end 24 perhaps ranges in width from 0.5 cm to 2 cm for the adult patient. For children and infants, the widths may be proportionally shorter, e.g., 1 cm for children and 0.5 cm f or infants.
- the proximal end 22 of the block 10 may have a width greater than 6 cm to accommodate patients with a very large oral cavity. The greater width of the improved blade 10 at its proximal end 22 provides the physician or other intubator an improved means for controlling the patient's tongue during the intubation procedure.
- the curvature of the arcuate body 20 should fall within certain limits.
- the conventional Macintosh blade has a rather steep curvature in order to facilitate passage over the tongue and to avoid depression of the tongue which might otherwise cause restriction of the visible aperture of the larynx.
- the conventional Macintosh is curved too much. Occasionally the physician or intubator can't see around the curvature of the Macintosh blade to view the larynx.
- the blade of the present invention has a gentle curvature.
- the patient be positioned to align an axis extending through the pharynx with an axis extending through the larynx, or in other words, the opening to the airway is widened by straightening the throat.
- the angle between the pharyngeal axis and the laryngeal axis is approximately 5° to 25°.
- the blade 10 of the present invention is designed to conform with this angle.
- a median axis M extending longitudinally through the bottom surface of the proximal portion 22 a of the arcuate body 20 intersects with a median axis A extending longitudinally through the distal portion 24 a of the body 20 to define an angle ⁇ .
- this angle ⁇ is between 5° and 25°, preferably approximately 15°. The more gradual curvature of the blade 10 of the present invention facilitates viewing the tip extension 32 when the blade 10 is inserted in the patient's throat.
- the blade 10 of the present invention is further improved by the addition of raised areas 40 defining grooves on the top surface 26 of the blade 10 , as seen in FIGS. 6 and 7.
- One of the grooves defined by the medial raised area 40 shown in the Figures may be used for guiding a tube over the top surface 26 of the blade 10 for insertion into the trachea, while the other groove preserves a line of sight to visualize the larynx and glottis.
- the blade may be further improved by the addition of a vertical wall 50 having its bottom edge attached to the edge of the proximal portion 22 a of the arcuate body 20 as shown in FIGS. 6 and 7.
- the vertical wall 50 may serve as a convenient location for mounting of the means for illumination 14 .
- the vertical wall When the vertical wall is thickened, it serves as a bite block to prevent the patient from damaging his teeth or preventing intubation by involuntarily biting the blade 10 or the tube.
- the additional raised area 40 shown adjacent to the vertical wall 50 in FIG. 6 might be used for insertion of a suction catheter to move any liquids in the mouth or throat obstructing visualization of the larynx.
- the patient's position is adjusted to align the airway for intubation.
- the blade 10 of the present invention is inserted medially towards the center of the mouth, by virtue of the width of the blade 10 approaching the width of the mouth.
- the tip of the Macintosh blade is inserted in the vallecula between the epiglottis and the base of the tongue, while the curved tip of the Miller blade is inserted behind the posterior edge of the epiglottis.
- the blade 10 of the present invention may be used in either manner, depending on the anatomy of the patient and the preference of the physician. Once the tip 30 is inserted in the proper location, the epiglottis is raised to open the airway to permit the insertion of the tube. The proper positioning of the tube in the airway is verified by x-ray or other means.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Surgery (AREA)
- Biomedical Technology (AREA)
- Medical Informatics (AREA)
- Optics & Photonics (AREA)
- Pathology (AREA)
- Radiology & Medical Imaging (AREA)
- Biophysics (AREA)
- Engineering & Computer Science (AREA)
- Physics & Mathematics (AREA)
- Heart & Thoracic Surgery (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Molecular Biology (AREA)
- Animal Behavior & Ethology (AREA)
- General Health & Medical Sciences (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Otolaryngology (AREA)
- Physiology (AREA)
- Pulmonology (AREA)
- Endoscopes (AREA)
Abstract
An improved laryngoscope blade for use with a conventional laryngoscope handle and conventional means for illumination. The improvements to the blade include a small reverse curve at the tip of the blade to better visualize the depth of insertion of the blade, include a greater width of the portion of the blade proximal to the handle to provide improved means for controlling the tongue, and include a more gradual curvature of the blade to better conform to the shape of the airway opening when the patient is properly positioned for laryngoscopy. The blade may also include a vertical wall which may be thickened to serve as a bite block, and raised areas to define grooves on the surface of the blade for insertion of an endotracheal tube and/or a suction catheter.
Description
1. Field of the Invention
The present invention relates to laryngoscopes, and particularly to an improved blade for a laryngoscope.
2. Description of the Related Art
While a laryngoscope may be used to visually examine the larynx, its more important function is to aid endotracheal intubation. The need for intubation may arise during a controlled situation, such as surgery, or in a crisis situation when the patient is unable to breathe adequately and requires a resuscitation bag or mechanical ventilation. During intubation, a flexible tube is inserted through the nasal or oral cavity, passed through the larynx, and into the trachea for the administration of gases. The larynx may be viewed as a chamber bounded superiorly by the epiglottis, inferiorly by the vocal cords which cover the opening to the trachea, anteriorly by the thyroid cartilage or Adam's apple, and posteriorly by a portion of the pharynx. The epiglottis is a lamella or leaf-like plate of cartilage which extends dorsally like a loose lid over the larynx, helping to protect the trachea by preventing food from entering the trachea during swallowing.
In order to intubate the patient, the intubator (either a physician or paramedic) must visualize the epiglottis and the vocal cords to watch the tube go past the vocal cords of the patient. The laryngoscope generally comprises a handle, a blade which is used to move the patient's tongue out of the way and to lift the epiglottis to expose the vocal cords, and a light source to illuminate the glottis and vocal cords.
The two most widely used blades in the current state of the art are known as the Miller blade and the Macintosh blade. The Miller blade is a substantially straight blade with a curved tip, the curve commencing approximate 2 inches from the end of the blade. The Macintosh blade is a blade which is curved for substantially its entire length (U.S. Pat. No. 2,354,471 issued Jul. 25, 1944). In use the Miller blade is inserted along the longitudinal axis of the larynx past the epiglottis to lift it enough to visualize the vocal cords and slip the tube through the cords into the trachea. The Macintosh blade is inserted on a combination of the axis of the oral cavity and the longitudinal axis of the larynx, the tip being placed in the vallecula, which are shallow depressions in the membranous folds and tissue between the epiglottis and the root of the tongue. By applying an upward pressure at the vallecula, the epiglottis is raised enough to visualize the vocal cords.
While intubation may be done with the existing blades, several shortcomings in the existing blades have prompted various efforts to improve the blades. Efforts to improve the curvature of the blade are shown in U.S. Pat. No. 5,003,962, issued Apr. 2, 1991 to Choi, and U.S. Pat. No. 5,406,941 issued Apr. 18, 1995 to Roberts. Choi describes a blade having three straight segments, the second segment at a 20 degree angle to the first, and the third at a 30 degree angle to the second. The Roberts patent describes a flat, flexible blade, having a cam attached to one side of the blade so the curvature may be adjusted by rotating the cam. U.S. Pat. No. 3,856,001 issued to O. C. Phillips Dec. 24, 1974 describes a Jackson or straight blade having a U-shaped cross-section and a tip similar to the Miller blade, curving about 2 inches from its end.
Efforts to improve the tip are shown in U.S. Pat. No. 4,573,451, issued Mar. 4, 1986 to Bauman, and U.S. Pat. No. 5,603,688 issued Feb. 18, 1997 to Upsher. The Bauman patent describes a blade made of plastic or metal, thinned or hinged at the tip, with a push rod and a ratchet to change the angle of the tip. Upsher's patent shows a blade having a hollow tube in the blade for insertion of the endotracheal tube, with an extension of one side of the tip to prevent the natural curve of the endotracheal tube from causing the end of the endotracheal tube to leave the field of vision after exiting the hollow tube in the blade.
Efforts to improve the illumination of the larynx and vocal cords are shown in U.S. Pat. No. 3,638,644 issued Feb. 1, 1972 to Reick, and U.S. Pat. No. 3,771,514 issued Nov. 13, 1973 to Huffman, et al. The Reick patent shows a light bulb in the handle with a plastic light conduit extending through the blade. The Huffman patent shows a one-piece handle and blade, the blade having a prism mounted thereon for reflecting and diffusing the light.
U.S. Pat. No. 5,036,835 issued Aug. 6, 1991 to Filli describes a blade which slides to adjust the length of the blade. U.S. Pat. No. 5,065,738 describes a sheath fitting over the blade to protect the patient's teeth, gums, oral mucosa and epiglottis from damage during insertion of the laryngoscope.
Various patents show a disposable blade, including European Patent 0184588 published Jun. 18, 1986, describing a disposable blade with a light source in the handle; International Patent 94/03101 published Feb. 17, 1994, describing a disposable blade with the light source in the blade; and International Patent 97/17885 published May 22, 1997, showing a disposable blade with a channel in the blade for the passage of fluids.
Construction techniques for incorporating a channel or path for a bulb and light cable or guide are shown in U.K. Patent 2,102,294 published Feb. 2, 1983, describing two L-shaped members pull together in overlapping fashion to form a channel for the light and cable, and U.K. Patent 2,102,679 describing a blade made by placing a fiber optic bundle in an injection mold and forming a plastic blade by injecting the mold with plastic.
None of the above inventions and patents, taken either singularly or in combination, is seen to describe the instant invention as claimed. Thus an improved laryngoscope blade solving the aforementioned problems is desired.
The present invention exploits the principle used by health care providers to widen the airway in preparation of intubation. When the head is in the normal anatomic position, the airway is narrow. It is therefore recommended that the intubator align the laryngeal and pharyngeal axes; unlike the present invention, in this position neither the Miller blade nor the Macintosh blade present the optimum angle for viewing and intubating the patient. Although the Macintosh blade is curved, the curvature is greater than the curvature of the airway, hence it does not permit optimal visualization of the vocal cords because the intubator can't see around the curvature of the blade. Moreover, with both the Miller blade and the Macintosh blade, the intubator has difficulty visualizing the tip of the blade, again due to the shape of the blade and the shape of the airway. Consequently the intubator has difficulty determining when the tip is in proper position.
Accordingly, it is a principal object of the invention to provide an improved laryngoscope blade which produces better visualization of the larynx through adjusting the curvature of the blade.
The present invention is a laryngoscope blade which is generally curved throughout its length. However, the curvature is more gradual than the curvature of the conventional Macintosh blade.
The invention also provides the tip of the blade with a small reverse curve at the tip of the blade, in order to permit better visualization of the position of the end of the blade.
The laryngoscope blade of the present invention further includes a proximal part which is contoured to the width and shape of the mouth, having a width of up to 6 cm., in order to provide better control of the tongue during laryngoscopy. This configuration is unlike the part of a conventional laryngoscope blade proximal to its connection with the handle, which is used to move the tongue away from the airway and prevent the tongue from obstructing visualization of the larynx. Therefore, present laryngoscope blades have a maximum width of approximately 2 cm.
It is a further object of the invention to provide improved elements and arrangements thereof for the purposes described which is inexpensive, dependable and fully effective in accomplishing its intended purposes.
These and other objects of the present invention will become readily apparent upon further review of the following specification and drawings.
FIG. 1 is a right side view of the improved laryngoscope blade according to the present invention.
FIG. 2 is a top plan view of the improved laryngoscope blade according to the present invention.
FIG. 3 is a top perspective view of the improved laryngoscope blade according to the present invention.
FIG. 4 is an end view of the improved laryngoscope blade according to the present invention.
FIG. 5 is an environmental perspective view of an alternative embodiment of the invention showing a “bite block”.
FIG. 6 is an end view of an alternative embodiment of the invention showing a “bite block” and raised areas on the surface of the blade defining grooves.
FIG. 7 is a top perspective view of an embodiment of the invention with a vertical wall and a raised area defining grooves on the blade.
Similar reference characters denote corresponding features consistently throughout the attached drawings.
The present invention relates to a laryngoscope with an improved blade. A conventional laryngoscope typically comprises a handle, a blade, and a light source. The blade is usually pivotally mounted on the blade so that the blade is substantially parallel to the handle when not in use, and is substantially perpendicular to the handle to form an L-shape in use.
A variety of arrangements may be used to provide a light source. Power for the light source is usually provided by batteries in the handle. The light source itself may be in the handle with a conduit mounted on the blade, or the light source itself may be mounted on the blade. The connector used to mount the blade may vary depending on the nature of the light source.
The improvement of the present invention does not relate to the handle, the light source, or the means connecting the blade to the handle. As shown more particularly in FIGS. 1 through 4, the present invention relates to the laryngoscope blade 10. The improved blade is designed to be used with a conventional handle 12 (shown in phantom in the drawings), means for illumination 14, and means 16 for connecting the blade 10 to the handle 12, all of which are well known in the prior art. Although the light source 14 is shown mounted on the top surface of the blade 10 in FIGS. 1 through 3, it will be appreciated that the light source 14 may be mounted alternatively on the edge of the blade 10, or in the handle 12 with a light-transmitting conduit towards the end of the blade 10, etc. The nature and location of the means for illumination 14 are not critical, provided that there are some means for illuminating the distal end of the blade 10 and an appropriate means 16 for connecting the blade 10 to the handle 12 adapted to the particular light source used.
The improved blade 10 has an arcuate body 20 having a proximal end 22 and a distal end 24, the body 20 being substantially flat, having a top surface 26 which is convex upwards as seen from a side view, and a bottom surface 28 concave downwards. The means 16 for connecting the blade 10 to the handle 12 is connected to the bottom surface 28 of the proximal end 22 of the body 20. The blade 10 has a tip 30 at the distal end 24 of the body 20, the tip 30 having a point of inflection as seen from a side view, most clearly seen in FIG. 1, and a short tip extension 32 being concave upwards. The tip extension 32 provides the physician or other person performing the intubation with a visual means for determining the depth to which the blade 10 has been inserted into the patient's throat, and can be rested on the top of the epiglottis, both features being an improvement on prior laryngoscope blades.
The top surface 26 and the bottom surface 28 of the blade 10 have a proximal portion 22a towards the proximal end 22 of the body 20 having a width of between 2 cm and 6 cm in the preferred embodiment, the proximal portion 22a having a substantially oblong shape, so the that proximal portion 22a conforms to the width of an adult patient's mouth. The top surface 26 and the bottom surface 28 have a distal portion 24a towards the distal end 24 of the body 20. The width of the blade 10 tapers from the proximal portion 22a to a width not greater than approximately 2 cm at the distal end 24, so that the distal end 24 may be inserted in the patient's throat.
It is contemplated that the blade 10 will be made in various sizes, with perhaps the width of the proximal portion of the body 20 ranging between 2 cm and 6 cm in 0.5 cm increments, while the distal end 24 perhaps ranges in width from 0.5 cm to 2 cm for the adult patient. For children and infants, the widths may be proportionally shorter, e.g., 1 cm for children and 0.5 cm f or infants. In an alternative embodiment, the proximal end 22 of the block 10 may have a width greater than 6 cm to accommodate patients with a very large oral cavity. The greater width of the improved blade 10 at its proximal end 22 provides the physician or other intubator an improved means for controlling the patient's tongue during the intubation procedure.
In order to derive full advantage from the improved tip 30 and tip extension 32 of the present invention, the curvature of the arcuate body 20 should fall within certain limits. The conventional Macintosh blade has a rather steep curvature in order to facilitate passage over the tongue and to avoid depression of the tongue which might otherwise cause restriction of the visible aperture of the larynx. However, the conventional Macintosh is curved too much. Occasionally the physician or intubator can't see around the curvature of the Macintosh blade to view the larynx.
The blade of the present invention has a gentle curvature. When intubating a patient, it is recommended that the patient be positioned to align an axis extending through the pharynx with an axis extending through the larynx, or in other words, the opening to the airway is widened by straightening the throat. When so positioned, the angle between the pharyngeal axis and the laryngeal axis is approximately 5° to 25°. The blade 10 of the present invention is designed to conform with this angle.
Viewing the blade 10 from the side, a median axis M extending longitudinally through the bottom surface of the proximal portion 22a of the arcuate body 20 intersects with a median axis A extending longitudinally through the distal portion 24a of the body 20 to define an angle θ. In the blade 10 of the present invention, this angle θ is between 5° and 25°, preferably approximately 15°. The more gradual curvature of the blade 10 of the present invention facilitates viewing the tip extension 32 when the blade 10 is inserted in the patient's throat.
The blade 10 of the present invention is further improved by the addition of raised areas 40 defining grooves on the top surface 26 of the blade 10, as seen in FIGS. 6 and 7. One of the grooves defined by the medial raised area 40 shown in the Figures may be used for guiding a tube over the top surface 26 of the blade 10 for insertion into the trachea, while the other groove preserves a line of sight to visualize the larynx and glottis.
The blade may be further improved by the addition of a vertical wall 50 having its bottom edge attached to the edge of the proximal portion 22a of the arcuate body 20 as shown in FIGS. 6 and 7. The vertical wall 50 may serve as a convenient location for mounting of the means for illumination 14. When the vertical wall is thickened, it serves as a bite block to prevent the patient from damaging his teeth or preventing intubation by involuntarily biting the blade 10 or the tube. The additional raised area 40 shown adjacent to the vertical wall 50 in FIG. 6 might be used for insertion of a suction catheter to move any liquids in the mouth or throat obstructing visualization of the larynx.
In operation, for an endotracheal intubation, the patient's position is adjusted to align the airway for intubation. Unlike the Macintosh and Miller blades, which are inserted in the right side of the patient's mouth, the blade 10 of the present invention is inserted medially towards the center of the mouth, by virtue of the width of the blade 10 approaching the width of the mouth.
In further contrast, the tip of the Macintosh blade is inserted in the vallecula between the epiglottis and the base of the tongue, while the curved tip of the Miller blade is inserted behind the posterior edge of the epiglottis. The blade 10 of the present invention may be used in either manner, depending on the anatomy of the patient and the preference of the physician. Once the tip 30 is inserted in the proper location, the epiglottis is raised to open the airway to permit the insertion of the tube. The proper positioning of the tube in the airway is verified by x-ray or other means.
It is to be understood that the present invention is not limited to the embodiments described above, but encompasses any and all embodiments within the scope of the following claims.
Claims (15)
1. An improved blade for a laryngoscope having a handle, comprising:
a) an arcuate body having a proximal portion including a proximal end and a distal portion including a distal end, the body being substantially flat, having a convex top surface and a concave bottom surface,
said proximal portion being configured and dimensioned to the width of a patient's mouth in order to depress and control the tongue of a patient during insertion of an endotracheal tube,
said distal portion tapering in width from the proximal portion to the distal end, the distal portion being configured and dimensioned to enter a throat of the patient in order to raise the epiglottis for insertion of the endotracheal tube,
wherein a median axis extending longitudinally through the proximal portion of the bottom surface of said arcuate body and a median axis extending longitudinally through the distal portion of the bottom surface of said arcuate body intersect to define an angle between and inclusive of 5 and 25 degrees;
b) means for connection to the laryngoscope handle connected to the proximal end of said arcuate body;
c) a tip at the distal end of said arcuate body, the tip having a point of inflection and a short tip extension from said point, the extension being substantially concave upwards; and
d) means for illuminating the distal end of said arcuate blade.
2. The improved blade for a laryngoscope according to claim 1 , wherein the top surface and the bottom surface of said arcuate body have a proximal portion having a width greater than 2 cm, the proximal portion having a substantially oblong shape, and a distal portion which tapers in width from the proximal portion to a width of not greater than 2 cm at the distal end of said arcuate body.
3. The improved blade for a laryngoscope according to claim 1 , wherein the top surface and the bottom surface of said arcuate body have a proximal portion having a width of between 2 cm and 6 cm, the proximal portion having a substantially oblong shape, and a distal portion which tapers in width from the proximal portion to a width not greater than 2 cm at the distal end of said arcuate body, wherein the proximal portion of said arcuate body is configured and dimensioned to the width of a patient's mouth and the distal portion is configured and dimensioned to enter the patient's throat.
4. The improved blade for a laryngoscope according to claim 1 , further comprising at least one raised area on the convex top surface of said arcuate body defining a plurality of grooves whereby the larynx may be visualized and whereby and endotracheal tube or suction catheter may be passed over the blade and inserted into the trachea.
5. The improved blade for a laryngoscope according to claim 4 , further comprising a vertical wall having its bottom edge attached to an edge of the proximal portion of said arcuate body.
6. The improved blade for a laryngoscope according to claim 5 , wherein said vertical wall is dimensioned and configured in thickness to serve as a bite block whereby the patient is prevented from damaging his teeth by biting said blade and from preventing intubation by biting the tube.
7. The improved blade for a laryngoscope according to claim 1 , wherein said means for connection to the laryngoscope handle is attached to the bottom surface of said arcuate body and pivotally mounts the blade to the laryngoscope handle so that the blade is substantially parallel to the handle when not in use and substantially perpendicular to the handle to form an L-shape in use.
8. An improved blade for a laryngoscope having a handle, comprising:
a) an arcuate body having a proximal portion including a proximal end and a distal portion including a distal end, the body being substantially flat, having a convex top surface and a concave bottom surface,
said proximal portion being configured and dimensioned to the width of a patient's mouth in order to depress and control the tongue of a patient during insertion of an endotracheal tube,
said distal portion tapering in width from the proximal portion to the distal end, the distal portion being configured and dimensioned to enter the throat of a patient in order to raise the epiglottis for insertion of the endotracheal tube,
wherein a median axis extending longitudinally through the proximal portion of the bottom surface of said arcuate body and a median axis extending longitudinally through the distal portion of the bottom surface of said arcuate body intersect to define an angle between and inclusive of 5 and 25 degrees;
b) means for connection to the laryngoscope handle connected to the proximal end of said arcuate body; and
c) means for illuminating the distal end of said arcuate blade.
9. The improved blade for a laryngoscope according to claim 8 , wherein the top surface and the bottom surface of said arcuate body have a proximal portion having a width greater than 2 cm, the proximal portion having a substantially oblong shape, and a distal portion which tapers in width from the proximal portion to a width of not greater than 2 cm at the distal end of said arcuate body.
10. The improved blade for a laryngoscope according to claim 8 , wherein the top surface and the bottom surface of said arcuate body have a proximal portion having a width of between 2 cm and 6 cm, the proximal portion having a substantially oblong shape, and a distal portion which tapers in width from the proximal portion to a width not greater than 2 cm at the distal end of said arcuate body, wherein the proximal portion of said arcuate body is configured and dimensioned to the width of a patient's mouth and the distal portion is configured and dimensioned to enter the patient's throat.
11. The improved blade for a laryngoscope according to claim 8 , further comprising at least one raised area on the convex top surface of said arcuate body defining a plurality of grooves whereby the larynx may be visualized and whereby an endotracheal tube or suction catheter may be passed over the blade and inserted into the trachea.
12. The improved blade for a laryngoscope according to claim 11 , further comprising a vertical wall having its bottom edge attached to an edge of the proximal portion of said arcuate body.
13. The improved blade for a laryngoscope according to claim 12 , wherein said vertical wall is dimensioned and configured in thickness to serve as a bite block whereby the patient is prevented from damaging his teeth by biting said blade and from preventing intubation by biting the tube.
14. The improved blade for a laryngoscope according to claim 8 , wherein said means for connection to the laryngoscope handle is attached to the bottom surface of said arcuate body and pivotally mounts the blade to the laryngoscope handle so that the blade is substantially parallel to the handle when not in use and substantially perpendicular to the handle to form an L-shape in use.
15. The improved blade for a laryngoscope according to claim 8 , wherein the distal end of said arcuate body includes a tip having a point of inflection and a short tip extension from said point.
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US09/654,222 USRE37861E1 (en) | 1998-03-26 | 2000-08-31 | Laryngoscope blade |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US09/048,068 US5888195A (en) | 1998-03-26 | 1998-03-26 | Laryngoscope blade |
| US09/654,222 USRE37861E1 (en) | 1998-03-26 | 2000-08-31 | Laryngoscope blade |
Related Parent Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US09/048,068 Reissue US5888195A (en) | 1998-03-26 | 1998-03-26 | Laryngoscope blade |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| USRE37861E1 true USRE37861E1 (en) | 2002-09-24 |
Family
ID=21952570
Family Applications (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US09/048,068 Ceased US5888195A (en) | 1998-03-26 | 1998-03-26 | Laryngoscope blade |
| US09/654,222 Expired - Lifetime USRE37861E1 (en) | 1998-03-26 | 2000-08-31 | Laryngoscope blade |
Family Applications Before (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US09/048,068 Ceased US5888195A (en) | 1998-03-26 | 1998-03-26 | Laryngoscope blade |
Country Status (5)
| Country | Link |
|---|---|
| US (2) | US5888195A (en) |
| EP (1) | EP1063914A4 (en) |
| AU (1) | AU3211499A (en) |
| CA (1) | CA2326521A1 (en) |
| WO (1) | WO1999048416A1 (en) |
Cited By (14)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20040167429A1 (en) * | 2003-02-20 | 2004-08-26 | Roshdieh Babak B. | Cutaneous biopsy device with handle and disposable tips |
| US20050054903A1 (en) * | 2003-09-04 | 2005-03-10 | Cantrell Elroy T. | Dual blade laryngoscope with esophageal obturator |
| US20060247497A1 (en) * | 2005-04-29 | 2006-11-02 | Gardner Glenn P | Instrument for direct laryngoscopy with a rigid blade and flexible fiberoptics |
| US20070129607A1 (en) * | 2005-12-07 | 2007-06-07 | Muhammad Ashfaque | Laryngoscope blade |
| US20070232862A1 (en) * | 2006-04-03 | 2007-10-04 | Dwight Herman | Laryngoscope blade |
| US20070287888A1 (en) * | 2006-06-09 | 2007-12-13 | Dp Medical | Integrated laryngoscope and suction device |
| US20080033249A1 (en) * | 2006-08-04 | 2008-02-07 | Carl Kaoru Sakamoto | Laryngoscope Blade |
| WO2009019703A2 (en) * | 2007-08-07 | 2009-02-12 | Truphatek International Ltd | Laryngoscope apparatus with enhanced viewing capability |
| US20100041953A1 (en) * | 2004-02-29 | 2010-02-18 | Truphatek International Ltd., | Metal laryngoscope blade with illumination assembly |
| US7744529B2 (en) | 2004-02-12 | 2010-06-29 | Carl Kaoru Sakamoto | Laryngoscope blade |
| US20110092774A1 (en) * | 2009-09-09 | 2011-04-21 | Dwight Herman | Laryngoscope blade |
| US8512234B2 (en) | 2011-04-07 | 2013-08-20 | Truphatek International Ltd. | Laryngoscope assembly with enhanced viewing capability |
| US8864661B2 (en) | 2011-01-27 | 2014-10-21 | Mayo Foundation For Medical Education And Research | Transoral retractor for robotic surgery |
| USD1048571S1 (en) | 2021-10-07 | 2024-10-22 | Masimo Corporation | Bite block |
Families Citing this family (44)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| USD413977S (en) * | 1998-05-26 | 1999-09-14 | Cranton George D | Laryngoscope blade |
| US6217514B1 (en) * | 1999-02-05 | 2001-04-17 | Gruhan Technologies, Inc. | Laryngoscope |
| US6901928B2 (en) * | 1999-05-04 | 2005-06-07 | Paul G. Loubser | Superglottic and peri-laryngeal apparatus for supraglottic airway insertion |
| US6231505B1 (en) * | 1999-09-20 | 2001-05-15 | Tyson Edward Martin | Laryngoscope blade |
| US6623425B2 (en) * | 2001-07-23 | 2003-09-23 | Cartledge Medical Products, Llc | Modified laryngoscope blade to reduce dental injuries during intubation |
| AU2003269450A1 (en) * | 2002-10-03 | 2004-04-23 | Etview Ltd. | Tube for inspecting internal organs of a body |
| US20050159649A1 (en) * | 2004-01-16 | 2005-07-21 | Patel Rajeev J. | Laryngoscope and associated method of intubating a patient |
| US20050240081A1 (en) * | 2004-04-22 | 2005-10-27 | The Cleveland Clinic Foundation | Laryngoscope blade |
| WO2006065271A2 (en) * | 2004-12-15 | 2006-06-22 | Embo-Optics, Llc | Point of infusion lighting device |
| AU2006232535A1 (en) | 2005-04-01 | 2006-10-12 | Welch Allyn, Inc. | Illumination assembly for use with vaginal speculum apparatus |
| US7909758B2 (en) * | 2006-10-31 | 2011-03-22 | Leon Shapiro | Apparatus for orotracheal intubation |
| IL179291A0 (en) * | 2006-11-15 | 2007-03-08 | Leonid Lukov | Intubation laryngoscope with two-sided blade |
| US20100198017A1 (en) * | 2009-01-30 | 2010-08-05 | Taps, Llc | Laryngoscope Blade |
| US9913577B2 (en) | 2010-09-28 | 2018-03-13 | Obp Medical Corporation | Speculum |
| EP2611356B1 (en) | 2011-07-11 | 2014-12-24 | Etview Ltd. | Endobronchial tube |
| US9084572B2 (en) | 2011-11-01 | 2015-07-21 | Michael J. Trakas | Collapsible laryngoscope |
| US9357905B2 (en) | 2012-06-01 | 2016-06-07 | Robert Molnar | Airway device, airway assist device and the method of using same |
| US9415179B2 (en) | 2012-06-01 | 2016-08-16 | Wm & Dg, Inc. | Medical device, and the methods of using same |
| EP2754384B1 (en) | 2013-01-10 | 2018-07-11 | Ambu A/S | Endobronchial tube with integrated image sensor and cleaning nozzle arrangement |
| US9918618B2 (en) | 2014-08-08 | 2018-03-20 | Wm & Dg, Inc. | Medical devices and methods of placement |
| US11147442B2 (en) | 2014-08-08 | 2021-10-19 | Wm & Dg, Inc. | Medical devices and methods of placement |
| US10722110B2 (en) | 2014-08-08 | 2020-07-28 | Wm & Dg, Inc. | Medical devices and methods of placement |
| US11633093B2 (en) | 2014-08-08 | 2023-04-25 | Wm & Dg, Inc. | Medical devices and methods of placement |
| US10420538B2 (en) | 2015-02-05 | 2019-09-24 | Obp Medical Corporation | Illuminated surgical retractor |
| US9867602B2 (en) | 2015-02-05 | 2018-01-16 | Obp Medical Corporation | Illuminated surgical retractor |
| US10881387B2 (en) | 2015-06-03 | 2021-01-05 | Obp Medical Corporation | Retractor |
| US10939899B2 (en) | 2015-06-03 | 2021-03-09 | Obp Medical Corporation | End cap assembly for retractor and other medical devices |
| ES2968069T3 (en) | 2015-06-03 | 2024-05-07 | Obp Surgical Corp | Retractor |
| US10722621B2 (en) | 2016-07-11 | 2020-07-28 | Obp Medical Corporation | Illuminated suction device |
| US10687793B2 (en) | 2017-07-18 | 2020-06-23 | Obp Medical Corporation | Minimally invasive no touch (MINT) procedure for harvesting the great saphenous vein (GSV) and venous hydrodissector and retractor for use during the MINT procedure |
| JP7349987B2 (en) | 2017-08-07 | 2023-09-25 | マクスウェル ワインマン, | laryngoscope |
| US11051682B2 (en) | 2017-08-31 | 2021-07-06 | Wm & Dg, Inc. | Medical devices with camera and methods of placement |
| US10278572B1 (en) | 2017-10-19 | 2019-05-07 | Obp Medical Corporation | Speculum |
| US10799229B2 (en) | 2018-02-20 | 2020-10-13 | Obp Medical Corporation | Illuminated medical devices |
| EP3755234A4 (en) | 2018-02-20 | 2021-11-17 | OBP Surgical Corporation | Illuminated medical devices |
| CN108992028A (en) * | 2018-07-10 | 2018-12-14 | 王庆元 | A kind of laryngeal mirror lens facilitating laryngeal mask |
| US10653307B2 (en) | 2018-10-10 | 2020-05-19 | Wm & Dg, Inc. | Medical devices for airway management and methods of placement |
| USD911521S1 (en) | 2019-02-19 | 2021-02-23 | Obp Medical Corporation | Handle for medical devices including surgical retractors |
| USD904607S1 (en) | 2019-05-07 | 2020-12-08 | Obp Medical Corporation | Nasal retractor |
| CN110960182A (en) * | 2019-11-26 | 2020-04-07 | 纳智医疗设备(徐州)有限公司 | Portable visual laryngoscope |
| US10959609B1 (en) | 2020-01-31 | 2021-03-30 | Obp Medical Corporation | Illuminated suction device |
| US10966702B1 (en) | 2020-02-25 | 2021-04-06 | Obp Medical Corporation | Illuminated dual-blade retractor |
| US11206973B1 (en) | 2020-09-14 | 2021-12-28 | Kenneth Hiller | Laryngoscope |
| US11497394B2 (en) | 2020-10-12 | 2022-11-15 | Wm & Dg, Inc. | Laryngoscope and intubation methods |
Citations (21)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US2354471A (en) * | 1943-08-18 | 1944-07-25 | Foregger Company Inc | Laryngoscope |
| US3638644A (en) * | 1969-03-05 | 1972-02-01 | Michael Elbert | Illuminated surgical speculum |
| US3771514A (en) * | 1971-06-29 | 1973-11-13 | Concept | Laryngoscope |
| US3856001A (en) * | 1973-08-24 | 1974-12-24 | O Phillips | Laryngoscope blade |
| GB2102294A (en) * | 1981-05-18 | 1983-02-02 | Heine Optotech Kg | Laryngoscope and improved blade therefor |
| GB2102679A (en) * | 1981-05-18 | 1983-02-09 | Heine Optotech Kg | Laryngoscope and improved blade therefor |
| US4556052A (en) * | 1983-05-17 | 1985-12-03 | Gustav Mueller Gmbh Und Co. Kg | Medical instrument with internal light source for illuminating body cavities |
| US4565187A (en) * | 1984-09-04 | 1986-01-21 | Soloway David J | Laryngoscope |
| US4573451A (en) * | 1984-11-08 | 1986-03-04 | Jack Bauman | Laryngoscope blade with a bendable tip |
| EP0184588A1 (en) * | 1984-12-11 | 1986-06-18 | Jack Bauman | Laryngoscope with disposable blade and light conductor |
| US4901708A (en) * | 1988-07-22 | 1990-02-20 | Lee Tzium Shou | Viewing laryngoscope |
| US5003962A (en) * | 1989-05-10 | 1991-04-02 | Choi Jay J | Laryngoscope with double-angle blade |
| US5036835A (en) * | 1990-04-27 | 1991-08-06 | Mesoud Filli | Adjustable sliding laryngoscope blade |
| US5060633A (en) * | 1990-08-31 | 1991-10-29 | Gibson Michael S | Laryngoscope blade |
| US5065738A (en) * | 1990-01-16 | 1991-11-19 | Dam David J Van | Laryngoscope blade sheath |
| US5095888A (en) * | 1990-07-09 | 1992-03-17 | Circon Corporation | Intubating stylet for a laryngoscope |
| WO1994003101A1 (en) * | 1992-07-28 | 1994-02-17 | William Lacey | Laryngoscope having removable blade assembly containing lamp |
| US5406941A (en) * | 1993-01-27 | 1995-04-18 | Roberts; James T. | Adjustable curvature laryngoscope blade |
| US5603688A (en) * | 1995-04-24 | 1997-02-18 | Upsher Laryngoscope Corporation | Laryngoscope including an upwardly curved blade having a downwardly directed tip portion |
| WO1997017885A2 (en) * | 1995-11-15 | 1997-05-22 | Bar Or David | Laryngoscope and disposable blade therefor |
| US5651761A (en) * | 1995-04-21 | 1997-07-29 | Upsher Laryngoscope Corp. | Laryngoscope including an endotracheal tube separation mouth and its method of use |
Family Cites Families (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| BE522807A (en) * |
-
1998
- 1998-03-26 US US09/048,068 patent/US5888195A/en not_active Ceased
-
1999
- 1999-03-26 AU AU32114/99A patent/AU3211499A/en not_active Abandoned
- 1999-03-26 WO PCT/US1999/006735 patent/WO1999048416A1/en not_active Application Discontinuation
- 1999-03-26 CA CA002326521A patent/CA2326521A1/en not_active Abandoned
- 1999-03-26 EP EP99914219A patent/EP1063914A4/en not_active Withdrawn
-
2000
- 2000-08-31 US US09/654,222 patent/USRE37861E1/en not_active Expired - Lifetime
Patent Citations (21)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US2354471A (en) * | 1943-08-18 | 1944-07-25 | Foregger Company Inc | Laryngoscope |
| US3638644A (en) * | 1969-03-05 | 1972-02-01 | Michael Elbert | Illuminated surgical speculum |
| US3771514A (en) * | 1971-06-29 | 1973-11-13 | Concept | Laryngoscope |
| US3856001A (en) * | 1973-08-24 | 1974-12-24 | O Phillips | Laryngoscope blade |
| GB2102294A (en) * | 1981-05-18 | 1983-02-02 | Heine Optotech Kg | Laryngoscope and improved blade therefor |
| GB2102679A (en) * | 1981-05-18 | 1983-02-09 | Heine Optotech Kg | Laryngoscope and improved blade therefor |
| US4556052A (en) * | 1983-05-17 | 1985-12-03 | Gustav Mueller Gmbh Und Co. Kg | Medical instrument with internal light source for illuminating body cavities |
| US4565187A (en) * | 1984-09-04 | 1986-01-21 | Soloway David J | Laryngoscope |
| US4573451A (en) * | 1984-11-08 | 1986-03-04 | Jack Bauman | Laryngoscope blade with a bendable tip |
| EP0184588A1 (en) * | 1984-12-11 | 1986-06-18 | Jack Bauman | Laryngoscope with disposable blade and light conductor |
| US4901708A (en) * | 1988-07-22 | 1990-02-20 | Lee Tzium Shou | Viewing laryngoscope |
| US5003962A (en) * | 1989-05-10 | 1991-04-02 | Choi Jay J | Laryngoscope with double-angle blade |
| US5065738A (en) * | 1990-01-16 | 1991-11-19 | Dam David J Van | Laryngoscope blade sheath |
| US5036835A (en) * | 1990-04-27 | 1991-08-06 | Mesoud Filli | Adjustable sliding laryngoscope blade |
| US5095888A (en) * | 1990-07-09 | 1992-03-17 | Circon Corporation | Intubating stylet for a laryngoscope |
| US5060633A (en) * | 1990-08-31 | 1991-10-29 | Gibson Michael S | Laryngoscope blade |
| WO1994003101A1 (en) * | 1992-07-28 | 1994-02-17 | William Lacey | Laryngoscope having removable blade assembly containing lamp |
| US5406941A (en) * | 1993-01-27 | 1995-04-18 | Roberts; James T. | Adjustable curvature laryngoscope blade |
| US5651761A (en) * | 1995-04-21 | 1997-07-29 | Upsher Laryngoscope Corp. | Laryngoscope including an endotracheal tube separation mouth and its method of use |
| US5603688A (en) * | 1995-04-24 | 1997-02-18 | Upsher Laryngoscope Corporation | Laryngoscope including an upwardly curved blade having a downwardly directed tip portion |
| WO1997017885A2 (en) * | 1995-11-15 | 1997-05-22 | Bar Or David | Laryngoscope and disposable blade therefor |
Cited By (23)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20040167429A1 (en) * | 2003-02-20 | 2004-08-26 | Roshdieh Babak B. | Cutaneous biopsy device with handle and disposable tips |
| US20050054903A1 (en) * | 2003-09-04 | 2005-03-10 | Cantrell Elroy T. | Dual blade laryngoscope with esophageal obturator |
| US6991604B2 (en) | 2003-09-04 | 2006-01-31 | Scope Co, Inc. | Dual blade laryngoscope with esophageal obturator |
| US7500948B2 (en) | 2003-09-04 | 2009-03-10 | Cantrell Elroy T | Dual blade laryngoscope with esophageal obturator |
| US7744529B2 (en) | 2004-02-12 | 2010-06-29 | Carl Kaoru Sakamoto | Laryngoscope blade |
| US8142353B2 (en) | 2004-02-29 | 2012-03-27 | Truphatek International Ltd. | Metal laryngoscope blade with illumination assembly |
| US20100041953A1 (en) * | 2004-02-29 | 2010-02-18 | Truphatek International Ltd., | Metal laryngoscope blade with illumination assembly |
| US7563227B2 (en) | 2005-04-29 | 2009-07-21 | Gardner Glenn P | Instrument for direct laryngoscopy with a rigid blade and flexible fiberoptics |
| US20060247497A1 (en) * | 2005-04-29 | 2006-11-02 | Gardner Glenn P | Instrument for direct laryngoscopy with a rigid blade and flexible fiberoptics |
| US20070129607A1 (en) * | 2005-12-07 | 2007-06-07 | Muhammad Ashfaque | Laryngoscope blade |
| US20070232862A1 (en) * | 2006-04-03 | 2007-10-04 | Dwight Herman | Laryngoscope blade |
| US7909757B2 (en) | 2006-04-03 | 2011-03-22 | Dwight Herman | Laryngoscope blade |
| US20070287888A1 (en) * | 2006-06-09 | 2007-12-13 | Dp Medical | Integrated laryngoscope and suction device |
| US20080033249A1 (en) * | 2006-08-04 | 2008-02-07 | Carl Kaoru Sakamoto | Laryngoscope Blade |
| US7955256B2 (en) * | 2006-08-04 | 2011-06-07 | Carl Kaoru Sakamoto | Laryngoscope blade |
| WO2009019703A2 (en) * | 2007-08-07 | 2009-02-12 | Truphatek International Ltd | Laryngoscope apparatus with enhanced viewing capability |
| WO2009019703A3 (en) * | 2007-08-07 | 2010-03-04 | Truphatek International Ltd | Laryngoscope apparatus with enhanced viewing capability |
| US20110060190A1 (en) * | 2007-08-07 | 2011-03-10 | Truphatek International Ltd. | Laryngoscope apparatus with enhanced viewing capability |
| US8251898B2 (en) | 2007-08-07 | 2012-08-28 | Truphatek International Ltd | Laryngoscope apparatus with enhanced viewing capability |
| US20110092774A1 (en) * | 2009-09-09 | 2011-04-21 | Dwight Herman | Laryngoscope blade |
| US8864661B2 (en) | 2011-01-27 | 2014-10-21 | Mayo Foundation For Medical Education And Research | Transoral retractor for robotic surgery |
| US8512234B2 (en) | 2011-04-07 | 2013-08-20 | Truphatek International Ltd. | Laryngoscope assembly with enhanced viewing capability |
| USD1048571S1 (en) | 2021-10-07 | 2024-10-22 | Masimo Corporation | Bite block |
Also Published As
| Publication number | Publication date |
|---|---|
| EP1063914A4 (en) | 2002-07-31 |
| CA2326521A1 (en) | 1999-09-30 |
| US5888195A (en) | 1999-03-30 |
| EP1063914A1 (en) | 2001-01-03 |
| WO1999048416A1 (en) | 1999-09-30 |
| AU3211499A (en) | 1999-10-18 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| USRE37861E1 (en) | Laryngoscope blade | |
| US10368732B2 (en) | Airway intubation device | |
| US5720275A (en) | Tracheal guide | |
| US7909757B2 (en) | Laryngoscope blade | |
| US5065738A (en) | Laryngoscope blade sheath | |
| US4901708A (en) | Viewing laryngoscope | |
| US5174283A (en) | Blind orolaryngeal and oroesophageal guiding and aiming device | |
| EP0500778B1 (en) | Blind orolaryngeal and oroesophageal guiding and aiming device | |
| US6629924B2 (en) | Enhanced endotracheal tube | |
| EP2756795A1 (en) | Intubation device | |
| US6494828B1 (en) | Laryngoscope | |
| US5984863A (en) | Pediatric laryngoscopic blade | |
| US8464710B1 (en) | Device for aiding intubation | |
| US20210023321A1 (en) | Bronchoendoscopic Intubation Guide Device | |
| US6764443B1 (en) | Laryngoscope | |
| US9084572B2 (en) | Collapsible laryngoscope | |
| US20210023319A1 (en) | Bronchoendoscopic Intubation Guide Device | |
| US20110092774A1 (en) | Laryngoscope blade | |
| US20070129607A1 (en) | Laryngoscope blade | |
| CN210673287U (en) | L-shaped narrow anatomical video pharyngoscope | |
| US7744529B2 (en) | Laryngoscope blade | |
| US20240252774A1 (en) | Stylet for endotracheal intubation | |
| CN215690784U (en) | Endotracheal tube interlock device | |
| GB2402342A (en) | A laryngoscope blade |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| FPAY | Fee payment |
Year of fee payment: 4 |
|
| FEPP | Fee payment procedure |
Free format text: PAYOR NUMBER ASSIGNED (ORIGINAL EVENT CODE: ASPN); ENTITY STATUS OF PATENT OWNER: SMALL ENTITY |
|
| FPAY | Fee payment |
Year of fee payment: 8 |
|
| FPAY | Fee payment |
Year of fee payment: 12 |