
COCHLEAR IMPLANTS
CONCERN OVER HSP PROPOSALS
There are calls to ensure the financial viability of audiology practices

OVER-THE-COUNTER HEARING AIDS What impact has the category had in the US and what's happening here?
50 YEARS OF INDUSTRY EDUCATION
A


PEAK BODIES ON HIGH ALERT OVER PROPOSED HSP CHANGES AS SURVEYS REVEAL CONCERNS
Several proposed reforms to the Hearing Services Program (HSP) have prompted calls to ensure that changes are cost-neutral to uphold the financial viability of audiology businesses providing the service. There are also concerns that if changes financially impact practices, communities could be adversely impacted and lose access to non-HSP services.
Hearing Business Alliance (HBA) and Audiology Australia (AudA) were commenting after the Department of Health and Aged Care released results on 11 July 2024 of its consultation with stakeholders and the public on proposed HSP changes. The department said feedback would inform updated service items and program standards.
Newly released data from 2023-2024 shows that annually
the program supports more than 806,000 Australians, delivers over 1.4 million services and fits about 436,000 hearing devices. Its voucher scheme has a network of more than 300 hearing providers who deliver subsidised hearing services and devices across about 3,000 locations nationwide.
Consultation findings revealed most respondents supported numerous proposed changes including changes to assessments, removing Audiological Case Management items, proposals to amalgamate client review and rehabilitation items, changes to assistive listening device (ALD) supply, replacements and spare devices, and eligibility criteria for fitting.
But the majority opposed or only partially supported proposed changes to fittings (72%) and

follow-ups (86%). Proposed changes to remote controls were also an area of concern with most against these while half were unsure about only allowing two replacements per ear in a five-year period.
Ms Jane MacDonald, HBA CEO, said alliance members appreciated the opportunity to contribute responses on phase one of the consultation. Service provision to HSP clients constituted a significant proportion of the work delivered
AHPRA BROADENS POWERS ON NON-REGISTERED PRACTITIONERS
New powers granted to Ahpra and the National Boards enable them to act against non-registered health practitioners if there are significant public safety concerns.
They now have greater power if there are concerns over non-Ahpra registered practitioners who previously fell outside their remit with the introduction of a new mechanism called interim prohibition orders (IPOs). IPOs can prevent unregistered practitioners – including suspended practitioners – from treating patients.
The measure by the Australian Health Practitioner Regulation Agency (Ahpra) and the National Boards is part of changes that the
regulator is ushering in during its most significant reforms since the National Law came into effect in 2010.
Ahpra CEO Mr Martin Fletcher said powers to issue IPOs about unregistered practitioners were an important safeguard for the wider health system. Some state and territory health complaints bodies already have this power.
“These powers will only be used in exceptional circumstances, when it is deemed there is a very real risk to the health and safety of individual patients or the wider community,” he said. “Whether people are consulting a registered practitioner or seeking help from a non-registered health worker, safe care relies on having
trust and confidence in everyone who is involved.
“Australia’s health system, as well as the reasons and ways people access it, has changed dramatically over the past 15 years. These reforms allow the regulation scheme to evolve, strengthening Ahpra and National Boards’ ability to protect the public and support practitioners.”
by most audiology businesses, she added.
She said it was difficult to comment on some of the proposed changes without financial modelling to reassure providers that changes would be cost-neutral, especially as it had been suggested that more than 50 claim items would be reduced to about 10 items.
“It is crucial to ensure financial viability for providers,” she told Hearing Practitioner Australia. (HPA). “Many smaller independent providers deliver other clinical services such as diagnostic and paediatric audiology, cochlear implant and vestibular services, and their local communities would be significantly negatively impacted should those providers be unable to continue practising.”
Some of the suggested changes
continued page 8

ON THE FRONTIER OF MÉNIÈRE'S DISEASE
Also, the public will have more information about practitioners on the public register, including if they use an alternative name to practise.
An Ahpra spokesman told HPA that as audiology was not registered under Ahpra, it was not listed as a protected title therefore was a profession not requiring registration.
ENT surgeon and neuroscientist Professor Jose Antonio Lopez-Escamez has moved from Spain to establish a research laboratory specialising in Ménière's disease at the Kolling Institute, the University of Sydney.
34
The HSP supports more than 806,000 Australians. Image: Peakstock/Shutterstock.

IN THIS ISSUE

An audiology king Audiology pioneer Dr Laurie Upfold OAM recalls how he helped build the profession in Australia.

Escaping APD
Dr Angela Alexander established the Auditory Processing Institute to train peers and help patients escape the disorder.


Educating the community
Penelope and Damien Woods from Brisbane give tips on educating GPs and the community about hearing health.
Changing lives
Microtia Atresia Australia founder Simone Cheadle has helped hundreds of children with the conditions – and their families.
CELEBRATING COCHLEAR IMPLANTS
More than one million people worldwide have benefitted from cochlear implants.
The story began in Australia where visionary Melbourne ENT surgeon Professor Graeme Clark, now 89, “wanted to fix ears” as a boy because he had a deaf father. His vision became reality and, 46 years ago after performing the first successful cochlear implant surgery, Prof Clark was so overcome he went quietly into the next-door lab and cried tears of joy.

The device has changed the way hearing loss is treated and began a revolution in hearing for severely to profoundly deaf people.
Many advances have occurred in the decades since to improve outcomes.
In this second edition of Hearing Practitioner Australia, we look at what’s new and what's on the horizon for this game-changing technology.
It’s been a privilege interviewing some of the many talented scientists, surgeons and audiologists involved in current research to propel the cochlear implant market forward. As we enter the era of optimisation, drug-eluting cochlear implants that release steroids to reduce inflammation, robots that insert the electrode array and totally implantable cochlear implants are among the new features that wearers could expect in the near future.
Continuing the cochlear theme, South Australian audiometrist Mr Dean Laird shows the beautiful Deafmetal jewellery, safety chains and accessories he sells for cochlear implant and hearing aid wearers to help them personalise their devices, reduce stigma and feel more comfortable.
There’s also a rich vein of history throughout this issue, including how audiology in Australia came about through the eyes of Dr Laurie Upfold, one of the national industry’s founding fathers. Dr Upfold, 90, received an OAM in the 2024 King’s Birthday Honours, providing an ideal moment to look back on his career and audiology in its infancy.
A feature on the 50th anniversary of The University of Melbourne’s audiology course – the nation’s first of its kind – also delves into some of the industry’s key milestones and looks at what might happen in the future. And there’s some great photos of a celebratory event that alumni attended to mark the occasion.
There’s plenty to read so enjoy!


HELEN CARTER Editor


UPFRONT

Just as HPA went to print, DR ANGELA ALEXANDER, a Queensland audiologist and auditory processing disorder expert, announced she was making a documentary about APD in people with hearing loss. She is heading to New Zealand to finish filming and plans to submit the doco to the Sundance Film Festival for January 2025. IN OTHER NEWS, researchers have produced supranormal hearing in mice by increasing the amount of neurotrophic factor neurotrophin-3 (Ntf3) in the inner
OFF THE BEATEN TRACK
Weird
French researchers have succeeded in directing floating objects around an aquatic obstacle course using only soundwaves. Their novel, optics-inspired method holds promise for biomedical applications such as non-invasive targeted drug delivery.
Wonderful
A scientific breakthrough in Israel has demonstrated the potential for speech using the power of thought only. In an experiment, a silent participant imagined saying one of two syllables. Depth electrodes implanted in his brain transmitted the electrical signals to a computer which vocalised syllables.
Wacky
Sound travels about five times faster underwater than on land, making sound localisation difficult for the human brain. By contrast, studies have shown that fish can locate sound sources such as prey or predators. A new study shows they possess a second, indirect hearing channel, where sound pressure gives fish the reference they need for directional hearing. The team also showed directional hearing can be fooled by reversing the acoustic pressure which in turn prompts fish to swim in the opposite direction.
ear. “We knew that providing Ntf3 to the inner ear in young mice increased the number of synapses between inner hair cells and auditory neurons, but we did not know what having more synapses would do to hearing,” said Dr Gabriel Corfas, director of Michigan Medicine’s Kresge Hearing Research Institute.
“We now show that animals with extra inner ear synapses have normal thresholds – what an audiologist would define as normal hearing – but they can process the auditory information in supranormal ways.” FINALLY, an interactive social inclusion program for aged care facilities, which may ultimately benefit the hearing health of
STAT
residents, has launched in Australia. The ‘Ciao!’ Program was initiated by the National Centre for Healthy Ageing in collaboration with Monash University, Peninsula Health and the Amplifon Foundation. It is being piloted in six residential aged care homes across Melbourne and provides residents with live interactive content such as chair-based yoga, virtual travel, therapeutic gardening and following the journey of a guide dog puppy in training. It provides opportunities for residents to connect with residents of other aged care homes through video technology and live online interactive sessions to enhance a sense of community.
Auditory anguish
Auditory processing disorder is estimated to impact 3% to 10% of the population, meaning up to 2.6 million Australians could be affected. Page 30.
WHAT'S ON
THIS month
OMOZ 2024
27 – 30 August
The conference will provide a forum for all researchers, clinical practitioners and health workers investigating and treating chronic ear disease and otitis media in Australia. omoz.com.au
NEXT
month
Complete calendar page 51.
WORLD CONGRESS OF AUDIOLOGY
19 – 22 September
Taking place in Paris for the event’s 36th edition, the scientific conference will bring together the world’s leading experts in hearing loss, tinnitus and vestibular disorders.
wca2024paris.com
hearingpractitionernews.com.au
Published by:
379 Docklands Drive, Docklands VIC 3008 T: 03 9690 8766
www.primecreative.com.au
Chief Operating Officer
Christine Clancy [email protected]
Publisher Sarah Baker [email protected]
Managing Editor Myles Hume [email protected]
Editor
Helen Carter [email protected]
Business Development Manager Luke Ronca [email protected]
Account coordinator Onella Siggins [email protected]
Client Success Manager
Salma Kennedy [email protected]
Design Production Manager
Michelle Weston [email protected]
Head of Design Blake Storey
Art Director Bea Barthelson
Subscriptions T: 03 9690 8766 [email protected] The Publisher
of the publisher.
MANY RESPONDENTS SHARED AUDA'S CONCERNS
continued from page 3
were welcomed, she said, such as simplifying administration processes around maintaining client devices and replacing lost devices but concerns were expressed about reducing the number of client reviews for unaided clients, capping the cost of remote controls, and removing client maintenance co-payments.
“HSP had communicated with providers that changes would be modelled to be cost-neutral to providers across a five-year voucher period,” MacDonald said.
“The department announced that an external consultant has begun work on modelling a possible fee structure for the revised service items, based on this consultation process.
“We note that only 132 survey responses were received from hearing health stakeholders, including service providers, professional bodies, industry groups and practitioners, and 60 from the public, including HSP clients.”
Ms Leanne Emerson, AudA CEO, said while the review was not yet complete, AudA noted with interest the survey results showing many respondents shared its concerns across key areas.
“In particular, extended fitting follow-up time frames, changes to remote control sourcing and device replacement caps, and lack of specific detail on key areas and their impact on quality care and business outcomes,” she told HPA.
“Audiology Australia continues to work with sector partners including the Hearing Health Sector Alliance to advocate for increased capacity for independent clinical
decision making, services that do not place unreasonable burden on audiologists or clients and policy that ensures effective treatment outcomes. As this process continues, we look forward to additional clarity with the release of updated services items and program standards later in 2024.”
Independent Audiologists Australia executive officer Ms Julie Watts said the organisation gave a detailed response and was pleased to see many members provided feedback. “We welcome the opportunity to contribute to creating a program that upholds evidence-based clinical service provision, and equitable participation for small independent providers and their patients. We look forward to more detail from the HSP on pricing, and further contributing to the revised schedule as it evolves,” she said. The department shared its proposal to improve the HSP standards with stakeholders on 20 February 2024. Two surveys collected feedback from hearing health stakeholders and clients/the public. Findings included:
• 81% supported proposed changes to assessments.
• Nearly 70% supported removing Audiological Case Management items.
• Respondents wanted clients to be appropriately referred for management when clinically indicated.
• 76% supported amalgamating client review and rehabilitation items into a new Clinical Session which 80% said should be available annually for most clients; 89% do not outsource rehabilitation

WITH PROVIDERS THAT CHANGES WOULD BE MODELLED TO BE COST-NEUTRAL TO PROVIDERS ACROSS A FIVEYEAR VOUCHER PERIOD.”
JANE MACDONALD, HEARING BUSINESS ALLIANCE
• Most comments (nearly 60%) indicated concern with proposals to extend the time frame of follow up.
• 77% supported changes to ALD supply; many suggested a separate ALD follow-up to align with separate fitting and follow-up services for hearing devices.
• 74% did not support/only partially supported proposed changes to remote controls, mainly due to them not being sourced under the proposed cap amount. Many suggested price should align with the process for hearing aids and ALDs.
• 84% supported changes to replacements.
• Most (94%) supported replacing statutory declarations with a lost device declaration.
• 56% did not support or were unsure about the proposal to allow only two replacements per ear over five-years before requiring a revalidated service and worried extra work would be needed for vulnerable clients in aqed care or with cognitive decline.
• 86% supported proposed changes to spare devices.
• Nearly 60% fully/partially supported proposed maintenance autopayments but were unsure about paying for repairs through a new separate item.
• There were mixed responses to removal of the maintenance co-payment.
• 55% supported proposed changes to device eligibility criteria to introduce a tool to gauge motivation to take up hearing loss advice/a hearing device;.
• 76% supported changes to eligibility criteria for refitting.
IPO'S CAN PREVENT PRACTITIONERS FROM TREATING PATIENTS
continued from page 3 and 84% would not outsource the clinical session.
Audiology is currently self-regulated but there is a consultation open examining whether it may be regulated in the future.
Ahpra registration is among seven options health ministers have put on the table as they consult on the future of audiology regulation. A final paper was due to be presented to health ministers on 27 July 2024 but has been delayed. Health ministers postponed their meeting to August 16.
A Queensland Government spokesperson said on 27 July that “the Audiology Regulatory Impact Statement (RIS) final report is currently being finalised”. Once
completed, stakeholders would be updated. Shortlisted options include the current model of self-regulation, national registration of the audiology profession through Ahpra’s National Registration and Accreditation Scheme (NRAS), and more targeted regulation of practitioners offering certain services.
The Ahpra changes complete a series of reforms to the Health Practitioner Regulation National Law aimed at strengthening public protection and improving operation of the NRAS.
Other key changes that started on 1 July 2024 include:
• establishing the process to renew a

Ahpra and the National Boards have new powers. Image: Valery Evlakhov/Shutterstock.
practitioner’s registration after a period of suspension has ended.
• extending powers for National Boards to exclude information about a practitioner from the public register if including it would pose a serious risk to the practitioner's health or safety, or the practitioner’s family members or associates. This includes risks such as those stemming from family, domestic or other violence.
• safety will be strengthened by making it easier for members of the public to verify a practitioner’s registration, with both a practitioner’s legal name and alternative name (if being used in practice) able to appear on the register.


IN BRIEF
AMA HONOUR
A co-founder of the Deadly Ears program, Queensland ENT surgeon Professor Chris Perry OAM, was inducted to the Australian Medical Association (AMA) Roll of Fellows for outstanding contributions to the association, medicine, the community and research. Prof Perry received the honour for “outstanding service to and leadership of AMA Queensland, for contribution to the federal AMA as a federal Councillor, and for distinguished service to medicine, particularly Indigenous health and ENT research”. A consultant surgeon in adult and paediatric otolaryngology head and neck surgery in Brisbane, he works in his private ENT practice, the Princess Alexandra Hospital and Queensland Children’s Hospital. He began attending remote Aboriginal communities in Cape York in 1982 and saw how otitis media, and its secondary deafness and education outcomes, was maintaining the poverty cycle. He secured federal funding to set up a program that engaged 20 ENT surgeons to travel to remote communities for three years which, in 2008, turned into Deadly Ears, Queensland Health’s response to reducing middle ear disease and hearing loss for First Nations children.
CHEMOTHERAPY HL
The first study to measure real-world listening challenges and hearing loss progression in cancer survivors over a long period of time has documented significant hearing difficulties in many testicular cancer survivors. The study, in the Journal of the American Medical Association Oncology, tracked 100 testicular cancer survivors with no hearing loss at baseline who received cisplatin-based chemotherapy. The median time since chemotherapy was 14 years. Comprehensive audiologic assessments revealed that 78% had audiometrically defined hearing loss and experienced significant difficulties in everyday listening situations. The men were, on average, 48 years old.
INTERPRETER SERVICE
A new central location for Bendigo Deaf Hub is part of a merger with Expression Australia, and assures its surviva – plus new services and facilities. Government funding for the hub ended in June 2024, but the merger has led to a new facility and additional services to improve access for the deaf and hard of hearing including a free onsite interpreter. Members of the deaf community can make a booking for the interpreter to assist with tasks that might otherwise be difficult such as medical appointments, parent teacher interviews or making accommodation bookings. Ms Rebecca Adam, Expression Australia CEO, said consultation with the Bendigo community was paramount.
“Equal access is a challenge in regional areas and we are committed to expanding on the wonderful work of the Deaf Hub services including education and employment pathways,” she said.
'COMPELLING EVIDENCE' OF ADULT-ONSET HEARING LOSS DEMENTIA RISK
A new review which analysed data from 50 cohort studies of more than 1.5 million people has provided “compelling evidence of adult-onset hearing loss being a robust and consistent independent risk factor for dementia”.
The systematic review and meta-analysis, the most comprehensive yet, suggested hearing loss significantly increases the risk of cognitive decline, dementia and Alzheimer’s disease. The researchers added there was “separate evidence that treating hearing loss with hearing aids may mitigate this association.”
They found hearing loss was associated with a 35% increased risk of incident dementia, a 29% increased risk of mild cognitive impairment and separately cognitive decline, and a 56% increased risk of Alzheimer’s disease dementia. The association with vascular dementia, however, was not statistically significant.
“Each 10-decibel worsening of hearing was associated with a 16% increase in dementia risk,” the researchers reported in the July edition of Ageing Research Reviews.
Furthermore, the impact of hearing loss on dementia did not vary significantly across dementia sub-types or other moderators such as baseline age or cardiovascular health.
cognitive decline, dementia, mild cognitive impairment and Alzheimer’s disease dementia.
“Adult-onset hearing loss is also potentially treatable, most often with hearing aids. Our findings suggest that this treatment may also reduce dementia risk.”
The study authors were from University College London including The Ear Institute, Johns Hopkins Medical Institutions, Baltimore USA and Edinburgh Napier University, Scotland.
They said theirs was the most comprehensive meta-analysis summarising the cohort evidence on adult-onset hearing loss as a risk factor for incident cognitive impairment and dementia, and included examining the evidence for dose-response, risk for various dementia subtypes, and other moderators.
“Our findings provide support to the possibility of a causal relationship between adult-onset hearing loss and dementia,” they added.
The systematic review and meta-analysis was the most comprehensive yet on the topic. Image: pikselstock/stock. adobe.com.
“This meta-analysis of cohort studies provided compelling evidence across diverse study settings and designs of adult-onset hearing loss being a robust and consistent independent risk factor for dementia,” they concluded.
“(The) cohort studies consistently support that adult-onset hearing

“First, our results are overall consistent in that despite heterogeneity between studies in population, methodology and type of incident cognitive outcome, most of the meta-analyses we conducted identified a statistically significant increase in risk across effect measures and cognitive outcomes, and even for those that were not significant, the magnitude of the effect consistently pointed towards risk increase.
“Second, we found evidence of a dose-response relationship. Both mild hearing loss and moderate-severe hearing loss were associated with increasing dementia risk, although the difference in risk increase by degree of hearing loss was not statistically significant.
“Third, our meta-analysis supported an appropriate temporal sequence between hearing loss and dementia by excluding studies with participants who already had dementia at baseline and excluding studies with less than two-year follow-up between hearing loss and subsequent dementia.”
They included cohort studies with participants who had no dementia and hearing assessments at baseline.
BUPA HEARING UNCHANGED AMID EXPANSION PLANS
Bupa has unveiled its vision for the future of healthcare including a roadmap to create a more connected and personalised journey across physical and digital channels and acquire integrated healthcare centres.
Its connected care strategy will initially focus on acquiring healthcare centres that offer integrated GP, allied health and pathology services. However, all optical and hearing services will continue to operate within Bupa’s optical and hearing stores through its partnership with Amplifon, rather than in integrated healthcare centres.
Unveiling its plan on 17 June 2024, Bupa said its initial focus would be on supporting people with mental health, type 2 diabetes, musculoskeletal health, oral and eye health issues.
“Over the coming years, Bupa plans to expand its provision footprint, building on its existing network of 178 dental clinics and 49 optical and hearing stores, to create a nationally distributed network of healthcare centres,” it said.
The healthcare centres will be available to anyone, not only Bupa Health Insurance customers.
Underpinned by current healthcare programs and networks of dental practices and optical stores, its

new strategy would bring together in-person and virtual care, supported by digital technology and partnerships.
Mr Adrian Kemp, director at Bupa Optical and Hearing, said its current 28 audiology clinics offered a range of audiology services throughout Australia through its partnership with Amplifon.
“We are excited about Bupa’s connected care strategy and are always looking for opportunities to optimise our national network of stores based on where we can best support and service local communities,” he said “All optical and hearing services will continue to operate within our
Bupa Optical and Hearing stores and through our partnership with Amplifon”.
A Bupa survey found more people were visiting an allied health practitioner compared to last year and while people preferred in-person appointments, there remained a strong desire for telehealth.
However Kemp said there were no immediate plans to expand its audiology offering into a digital or telehealth platform.
Mr Nick Stone, Bupa APAC CEO, said the new strategy was about bringing to life its vision to create personalised and seamless healthcare journeys for customers and the wider community.
“One of the biggest pain points for customers going through the healthcare system is how fragmented it is," he said.
"That’s why we’re working to connect care physically and digitally to remove barriers and increase affordability and convenience.
"We are building on our current network of dental practices, optical and hearing stores to give our members a truly connected health journey.”
AUSTRALIA’S MOST-TRUSTED HEARING PROVIDERS REVEALED
The nation’s most-trusted hearing care providers have been announced in Reader’s Digest magazine’s 25th annual Trusted Brands awards survey.
Hearing Australia won the hearing services category, with Specsavers and Amplifon Hearing Care Professionals receiving ‘highly commended’ awards.
For Specsavers Audiology Australia, this was the third year running it had received the ‘highly commended’ award in the hearing services’ category, while Specsavers Audiology New Zealand was highly commended for the second time in the New Zealand survey.
The annual survey is based on independent market research which brings together consumer opinions on leading brands across 68 categories in Australia and 67 in New Zealand.
This year, 4,300 Australians and 1,800 New Zealanders of a mixed
demographic were asked to rate their levels of trust in well-known brands.
Mr Tom Craw, Specsavers managing director of audiology Australia and New Zealand, welcomed the announcement.
“We’re thrilled to have been recognised as a ‘highly commended’ hearing services brand in both Australia and New Zealand,” he said.
“We’re committed to delivering hearing care with the same high-quality expertise and unbeatable value for money that Specsavers has long been known for. Receiving such great feedback in this prestigious consumer survey is a fantastic reminder that we’re delivering on our commitment.
“This acknowledgement is a testament to all our partners and store teams who work tirelessly every day to ensure that expert hearing care is available for all Australians and New Zealanders.”

Ms Louise Waterson, Reader’s Digest editor-in-chief, presents the award to Mr Stephen Tambouras, audiology partner relationship manager for Specsavers Australia. Image: Reader’s Digest.
Bupa operates 28 audiology clinics and has a partnership with Amplifon to provde the service. Image: Bupa.
PLAN TO CUT RED TAPE FOR OVERSEAS-TRAINED MEDICAL SPECIALISTS
The Medical Board of Australia (MBA) has released new details of its plan to fast-track certain internationally qualified medical specialists, including ENT surgeons, into the national health system without the need to sit exams.
The consultation is part of major workforce reforms following the ‘Kruk Review’ into removing “unnecessary regulatory barriers” faced by internationally qualified health professionals. It’s hoped cutting red tape will make Australia a more attractive destination for foreign health professionals and alleviate workforce pressures, leading to better healthcare for the population.
The MBA has released a draft consultation closing 3 July 2024 to meet reform deadlines set by Australia’s health ministers. The proposed fast-track pathway uses an existing provision in the National Law and will sit alongside the existing specialist medical college assessment system which will remain in place for specialist international medical graduates (SIMGs) who are not eligible for the expedited pathway.
The board said the expedited pathway would recognise specific overseas specialist medical qualifications and grant

doctors.
“The board, with input from the Australian Medical Council and specialist medical colleges, will develop and publish a list of qualifications that it considers are substantially equivalent or based on similar competencies to an approved specialist qualification for the specialty,” the consultation paper stated.
“The expedited pathway will not require a college assessment of the individual.” However, initial conditions on their registration will be imposed as a safeguard while the new recruits are inducted into Australia’s healthcare system.
GPs, anaesthetists, obstetricians and
Image: Ananass/stock. adobe.com.
gynaecologists, and psychiatrists are the priority specialties for now, with the fast-track pathway targeted to start for GPs in October 2024, and December 2024 for other priority medical specialties.
“[The] proposed changes to the registration standard aim to make the pathways to specialist registration clearer, establish the expedited pathway, remove outdated regulatory barriers and improve workforce flexibility, while maintaining standards,” the MBA said.
Ahpra and the MBA have set up a taskforce to develop the new expedited pathway, with MBA consulting the specialist colleges for the priority medical specialities to finalise the list of qualifications that will be the gateway to fast-track registration.
The board’s SIMG Taskforce lead, Dr Susan O’Dwyer, encouraged all agencies and individuals involved in recruiting and employing SIMGs to take part in the consultation.
“Australia has a complicated health system with shared responsibilities and accountabilities across agencies. We also share many common goals – most importantly, to enable safe medical care for Australians who need it, when they need it,” she said.
HEARING LOSS FIFTH MOST-COMMON LONG-TERM CONDITION
Deafness or hearing loss is the fifth most common long-term or chronic health condition in Australians, a new report from the Australian Institute of Health and Welfare (AIHW) has revealed.
Australia’s health 2024 found that an estimated 3.9 million people – one in six Australians or 15.5% of the population – were living with a chronic ear problem in 2022.
The most common ear condition was complete or partial deafness which affected 2.4 million people (9.6% of the population.)
The institute’s 19th biennial health report, released 2 July 2024, said deafness or hearing loss was ranked fifth out of 72 selected long-term health conditions. Anxiety topped the list at 4.8 million people (18.9%) followed by back problems (4 million people, 15.7%); depression (3.2 million people, 12.4%) and asthma (2.8
million people, 10.8%).
But for our First Nations people, ear and hearing issues ranked higher in the list of chronic health problems that lasted more than six months. Ear/hearing problems were the third most reported long-time health condition in First Nations people in 2018–2019 behind eye/sight problems and asthma. This translated to 114,000 Aboriginal and Torres Strait Islanders having ear/hearing problems or 14% of the Indigenous population.
Overall, long-term ear conditions were naturally more common in older people: half (49.5%) of people aged 75 and over self-reported having these conditions compared with 2.8% of those aged 0–14.
And while 61% of the population or 15.4 million people had one long-term health condition in 2022, 38% or 9.7 million had two or more conditions.
The report predicted the number of

Australians with dementia would more than double by 2058 to 849,300 people.
“In 2023, dementia was the second leading cause of disease burden overall, and the leading cause of burden for people aged 65 and over,” it stated. “In 2022, dementia was the second leading cause of death overall (9% of deaths), and the leading cause of death among Australians aged 65 and over.”
The report says one in six Australians have a chronic ear problem. Image: blvdone/stock.adobe. com.
Initial conditions will be imposed while the overseas recruits are inducted into the health system.
NEW HEAD OF ACAUD INC HAASA PLANS TO GROW THE ORGANISATION
New CEO of the Australian College of Audiology incorporating Hearing Aid Audiology Society of Australia, Mr Miguel Diaz, plans to grow the recently-merged organisation and the promotion of good hearing health.


Diaz previously worked in the health sector, most recently as CEO of Parkinson’s Queensland, and in a senior role with Camp Quality Australian children’s cancer charity. He is currently chair of the board of Health Consumers Queensland.
He started at ACAud inc HAASA on 11 June 2024 and said the opportunity to grow the body was what attracted him to the role.
“With around 3.9 million Australians experiencing some form of hearing loss, there’s an opportunity for ACAud inc HAASA to make a significant difference to the hearing health of Australians by promoting best practice across the hearing industry and advocating for improved access, affordability, equity and awareness,” he said “I’m looking forward to working with our members and the industry to promote good hearing health.”
Diaz replaced Ms Jane Hedger, former ACAud CEO, who left the college in May 2024 for a role outside the hearing health sector.
ACAud and HAASA announced on 13 March 2024 they would amalgamate to form a stronger organisation for enhanced advocacy, member support and client services. HAASA’s 130 audiometrist members were moved into the ACAud database of 875, 75% of whom were audiometrists and the rest audiologists, creating an organisation of 1,005 members.
Diaz said the amalgamation became official on 1 July and was working well.
“The new trading name is ACAud incorporating HAASA and the new logo is being finalised,” he said.
The week after he started in his new role he flew to Canberra for a two-day meeting with Hearing Health Sector Alliance colleagues, Department of Health representatives and advisor to the Minister for Health and Aged Care, Ms Aria Bolkus.
HEARING HEALTH SECTOR ALLIANCE RE-ELECTS CHAIR AND CHOOSES NEW DEPUTY
Australia’s Hearing Health Sector Alliance (HHSA) has re-elected Ms Jane MacDonald as chair, and chosen a new deputy chair, Audiology Australia CEO Ms Leanne Emerson.
Emerson replaces Ms Jane Hedger, former Australian College of Audiology (ACAud) CEO, who left the college in May 2024.
MacDonald, a Mildura-based audiologist and CEO of Hearing Business Alliance (HBA), was elected to serve HHSA for a second year when the organisation met in Canberra on 21 June 2024 for a two-day meeting.
Alliance members also met Mr Miguel Diaz, the new CEO of the Australian College of Audiology incorporating the Hearing Aid Audiology Society of Australia.
HHSA comprises 16 organisations and represents consumers, professionals, research and industry.
“The constructive and collaborative approach of the HHSA allows us to work closely with the Department of Health and Aged Care to support Australians living
with hearing and ear related challenges,” MacDonald said. She said the meeting agenda included issues covering HHSA priorities. To achieve improved hearing health outcomes and address challenges the priority areas are to:
• Advocate for the very best hearing health care and support for all people who experience hearing difficulty.
• Close the gap in ear and hearing health for First Nations people.
• Increase support for aged, vulnerable, disadvantaged Australians and communities.
• S ignificantly improve the rural and regional hearing health care workforce.
• Enhance and focus nationally funded research to achieve real, targeted impact. In her role as HBA CEO, MacDonald also met with Mr Bruce Billson, the Australian Small Business and Family Enterprise Ombudsman. They discussed issues which have a greater impact on small to medium independent audiology businesses and she said it was helpful to gain insights from him.
HEARING INDUSTRY SHINES
IN KING’S BIRTHDAY
HONOURS

A founding father of audiology in Australia, Dr Laurence John Upfold, has been recognised in the 2024 King’s Birthday Honours List, receiving a Medal of the Order of Australia (OAM) “for service to people who are deaf or hard of hearing”.
As one of the first audiologists in Australia and a pioneer in the field, he helped to establish the profession, urged university training in Australia and was a founding member of Audiology Australia (turn to page 18 for an in-depth article on his career).
Others in the field to receive King’s Birthday Honours included Mr Alexander John Clarke from Balcatta in WA who received an OAM “for service to people who are deaf or hard of hearing, and to the community”.
According to Deafness Council WA, Clarke has had a hearing impairment from an early age and has worked
tirelessly in the community for people with disabilities. He dedicated four years to the Ministerial Advisory Board for Disabilities WA and represented Australia at the worldwide Deaf and Blind conference in 2007.
Dr George Patrick Bridger from NSW was appointed a Member of the Order of Australia (AM) “for significant service to medicine through otolaryngology head and neck surgery”, while The Royal Victorian Eye and Ear Hospital’s board chair Dr Sherene Devanesen OAM received an AM for her service to community health through governance and administrative roles.
Hearing Australia non-executive board director, Professor Sharon Goldfeld, was also appointed an AM for “significant service to paediatric medicine as a clinician and academic, and to public health research”.
Leanne Emerson (left) and Jane MacDonald are the respective deputy chair and chair. Image: Jane MacDonald.
The Medal of the Order of Australia. Image: Supplied.
New ACAud incorporating HAASA CEO Miguel Diaz. Image: Miguel Diaz.
HEARING AUSTRALIA ANALYSIS OF HEARING LOSS IN INDIGENOUS CHILDREN
One in four First Nations children has undiagnosed ear disease, and one in five has undiagnosed hearing loss, an alarming new analysis of clinical findings has revealed.

Hearing Australia recently analysed the hearing assessments of 19,000 First Nations children across Australia as part of its Hearing Assessment Program – Early Ears (HAPEE).
It released the data on 3 July 2024, with key findings including:
• more than 26% of children assessed had undiagnosed ear disease
• 20% had undiagnosed hearing loss
• children under age two had more ear trouble than older children
• those in very remote locations had more problems than those in regional or metropolitan areas.
Otitis media in Aboriginal and Torres Strait Islander children remains among the highest globally and there is overwhelming evidence that hearing loss in young children can impact their learning and development.
“The good news is we are making headway in seeing children and getting them the help they need,” said Yorta Yorta woman Ms Kirralee Cross from Hearing Australia’s First Nations Services Unit.
“In 2022-2023, we assessed 14,435 First Nations children, the most in any year since the HAPEE program began in 2019.
“The data shows that while 60% of children have better hearing health when seen at a follow-up appointment, more needs to be done to improve community awareness of the importance of ear and hearing health.”
Cross said there needed to be a paradigm shift to tackle otitis media among First Nations children.
AUDIKA: ONE-QUARTER OF AUSSIES NEGLECT THEIR HEARING
More than one-quarter of Australians neglect their hearing because they “don’t understand and know where to start”, and more than half believe there is stigma around hearing loss, a survey of 1,005 adults suggests.
The nationwide online survey, commissioned by Audika which has more than 300 hearing clinics nationwide, shows Australians prioritise their sight over hearing, despite most (77%) knowing someone who is hard of hearing.
Most respondents (86%) ranked sight as their most important sense followed by hearing (69%) and this was reflected in which sense they cared for more, with 73% admitting that between hearing and sight, their hearing was the most neglected.
While the majority (80%) claimed they had ‘a little’ understanding of hearing loss, 27% said they neglected their hearing because they don’t understand and know where to start.
More than half (59%) thought there was stigma surrounding hearing loss and this increased among respondents aged 18-24 (61%) and 50-64 (64%). It declined slightly among those aged 65 and over (55%) and dropped to 40% for senior respondents.
Ms Mackenzie Arnold, an Audika ambassador and goalkeeper for the Australian women’s soccer team, recently discussed her experience with hearing loss. She

admitted there was stigma around avenues for addressing hearing loss that, as a child, prevented her from seeking treatment.
“Despite my brother having hearing loss since childhood, I convinced myself mine was not bad enough until early last year, and he was my biggest driver in seeking help,” she said.
“Since addressing my hearing loss, I have noticed a great change in the quality of my life, and I want to inspire others to feel comfortable to get their hearing checked earlier.”
NSW respondents were the most inclined among those surveyed to agree there was stigma around hearing loss (65%) compared to 58% in Queensland and Victoria, and 50% in Western Australia.
The survey was conducted by independent research services provider PureProfile in February 2024.
MEDICAL BOARD RELEASES NEW ENT WORKFORCE DATA

There were 566 otolaryngologists registered to practise in Australia in 2024, with more than half concentrated in just two states, the latest Medical Board of Australia report shows.
“Ear infections are common in children but for First Nations children they typically occur more often, start very early in life and last longer. There’s an urgent need for action at many levels – from the health system, service providers, practitioners and parents/ caregivers,” she said.
Herjua/stock. adobe.com.
Registrant data from 1 January 2024 to 31 March 2024 reveals six more specialists were performing otolaryngology-head and neck surgery nationwide in this quarter than the previous quarter, October to December 2023.
More than half (57%) were concentrated in just two states; NSW has 181 ENT specialists and Victoria has 140.
Queensland has the next largest concentration at 114 followed by 52 in Western Australia, 49 in South Australia, nine in the Australian Capital Territory, seven in Tasmania and four in the Northern
Territory. Ten had no principal place of practise.
Maldistribution and shortages in the ENT workforce are an ongoing issue.
They were previously highlighted in the National Health Workforce Dataset (NHWDS) Medical Specialties report 2016 which revealed that 460 otolaryngologists were employed in Australia, of whom 81.5% worked in the private sector. Most, 85%, were located in cities.
More recent data from The Australian Institute of Health and Welfare from December 2023 revealed that median waiting times for elective surgery for myringoplasty/tympanoplasty jumped from 259 days in 2021–2022 to 283 days in 2022–2023. This was nearly a three month longer wait than five years ago.
Mackenzie Arnold has hearing loss. Image: Audika.
A Hearing Australia audiologist performing an audiometry test on a First Nations child. Image: Hearing Australia.
Maldistribution of ENT surgeons in the Australian workforce is an ongoing issue. Image:
How GPs are handling hearing loss patients
An updated guide for Australian GPs urges opportunistic hearing assessment rather than annually screening everyone over 65. HPA dissects the latest ‘Red Book’ recommendations so hearing professionals can understand how doctors will detect hearing loss and handle referrals.
Anew edition of the book that guides Australian GPs in preventive practice has scrapped a previous recommendation for hearing screening every 12 months in people aged over 65 in favour of opportunistic assessment in specific populations.

The 10th edition of the RACGP's Red Book states “screening for hearing loss is generally not recommended in asymptomatic adults aged 50 or over”, based on the US Preventive Services Task Force recommendation statement.
Instead, its new recommendation, based on current evidence for those over 50, is for doctors to do opportunistic assessment of hearing in patients who present with conditions that may be associated with hearing loss.
These include children with speech or behavioural concerns, chronic ear infections or glue ear, and adults with perceived hearing loss or concerns. It states it is important to assess hearing in these individuals.
Other specific populations at greater risk of hearing loss, also appropriate for opportunistic screening, include older people, people who work in loud environments, those who listen to loud music and use headphones for music or gaming, First Nations children, Aboriginal and Torres Strait Islander people, patients with a family history of hearing loss and people from refugee-like backgrounds.
“In Australia, rates of chronic suppurative otitis media and cholesteatoma are much higher in the adult refugee population than in the broader Australian population,” the book states. “In addition, refugee children and adolescents may have missed screening for hearing problems.”
The Royal Australian College of GPs (RACGP) launched the 10th edition of its ‘Red Book’ Guidelines for preventive activities in general practice for GPs on 28 June 2024.
It says audiometry is best practice for a thorough assessment in these groups but hearing loss can also be assessed through single-question screening, asking: ‘Do you have difficulty with your hearing?’ or longer patient questionnaires such as the hearing handicap inventory screening HHIE questionnaire for the elderly.
“Hearing assessments such as whispered voice and finger rub are no longer recommended because results can be variable as they are user-dependent,” it states.
Dementia, hearing loss and hearing aids
The book broaches dementia, hearing loss and hearing aids in a section on risk reduction interventions for cognitive decline and dementia, stating, “there is insufficient evidence to recommend the use of hearing aids to reduce the risk
of cognitive decline and/or dementia”.
But it adds: “It is important for dementia patients and their carers to understand that there is a problem with cognition that needs management, and the concept of secondary prevention (ie. slowing the progression of the disease) can then be introduced (e.g. smoking cessation, correction of hearing impairment, optimal management of other cardiac risk factors, diet and exercise).”
A new addition to the book states general population screening for dementia is strongly not recommended. But it adds “hearing loss is a risk factor associated with dementia” and “screening followed by provision of hearing aids should be offered to older people for timely identification and management of hearing loss”.
Other recommendations re-stated from the 9th edition include that:
ABOVE: The Red Book is widely accepted as the main guide for preventive care in Australian general practice.
• all newborns should have universal hearing screening and GPs should ensure parents of newborn infants are aware of the universal neonatal hearing screening program in their relevant state and territory and have had their newborn screened for congenital hearing impairment.
• non-pharmacological approaches to the prevention of falls in older adults should include managing hearing impairment and referring for audiology assessment.
• additional time may be needed for Aboriginal and Torres Strait Islander women’s first antenatal visit if they have hearing impairment requiring the use of Auslan.
The book says although the prevalence of hearing loss tends to increase with age, it can affect people of all ages, with significant consequences on the physical, functional and mental health of the individual.
It says causes include age-related hearing loss; exposure to loud environments, including occupational environments (eg construction sites, concert venues, bars, nightclubs); congenital or early onset childhood hearing loss; complications from diseases such as measles, meningitis, rubella and mumps; genetics; ototoxic drugs that damage the inner ear and smoking.
“GPs are well placed to detect, diagnose and provide advice to help prevent hearing loss,” the book states.
It recommends that to help prevent hearing damage, GPs advise patients to avoid loud or sustained excessive noise, use hearing protection in high-noise environments, use volume controls for personal devices as necessary and avoid children being exposed to cigarette smoke.
High rates of persistent otitis media in infancy and childhood are associated with hearing loss across the life course for Aboriginal and Torres Strait Islander people and it advises GPs to refer to specific recommendations in the RACGP’s National guide to a preventive health assesment for Aboriginal and Torres Strait Islander people
The Red Book says vaccinations, which may reduce incidence of acute otitis media and/or acquired hearing loss, include annual influenza vaccination (inactivated virus) in anyone aged six months or over; rubella, measles, Haemophilus influenzae type b and meningococcus in children younger than 15 years; and pneumococcal conjugate vaccination (13vPCV) during infancy.
Preventive activities for pregnant women include offering testing for rubella immunity and syphilis serology to prevent infections that may lead to congenital hearing loss, it adds.
A ‘Rey’ of sunshine for the NT

REY DAYAP is Specsavers’ first audiologist based in the Northern Territory. Darwin born and bred, he returned home after seven years in Melbourne to provide Territorians with the unique Specavers brand of style, value and expertise.
Specsavers has more than 300 stores offering audiology nationwide but until now, none have operated in the Northern Territory’s Top End. That changed when The University of Melbourne-trained audiologist Mr Rey Dayap decided to return to his roots, paving the way for himself and hopefully others.
Dayap’s happy demeanour and easy-going nature lend themselves to the laid-back feel of Darwin and the NT.
“I’ve had customers say, ‘you know what I like about you? You’re local and you came back’,” Dayap says. “In a way I feel like a pioneer, and it comes with challenges and opportunities. One challenge is that before we provided audiology services in the NT we didn't advertise Specsavers Audiology, so when we did open we had people come in and say, ‘Oh I didn’t know Specsavers did hearing’. However, now we offer audiology services, we're advertising strongly, and people are telling me they’ve seen the ads on TV.”
While advertisements are bringing in some customers, Dayap says word of mouth from satisfied customers is proving a good drawcard with people referring friends.
“The business is slowly growing from word-of-mouth which means I’m doing something right if people are recommending me to their friends and family,” he says.
However, the bulk of his patients come from hearing screenings offered to optometry customers in store on an iPad as part of their customer journey.
After growing up in Palmerston, a satellite city of about 33,000 people 20 kilometres from Darwin, Dayap moved to Melbourne to study a Bachelor of Music majoring in composition at the University of Melbourne.
“I knew I wanted to do something in that field, and work with people. I’d been thinking about music therapy but after finishing in 2015 I changed my mind, as talking to friends who were doing it, I felt it wasn’t for me,” he recalls. Friends who were studying speech pathology, and his mother being
diagnosed with hearing loss when he was at university, gave him some exposure to audiology.
“When I first went into audiology, Mum said it was all because of her, and while it wasn’t exactly, I let her have that,” he says.
“I could see the impact and combined with my interest in sound, music and helping people it all clicked. I found linguistics fascinating, and a friend nudged me into thinking about audiology. I took a year off between honours and masters to consider if this was what I wanted to do but it was and I did my Masters in Audiology from 2017 to 2018.”
More than 200 days in outback communities
After graduation, Dayap was open to going anywhere for work. His top three places were Darwin, Hobart and Toowomba near friends but his recruitment agency was keen on Darwin.
“I moved home and worked with Hearing Australia for nearly five years,” he says. “I had one ‘normal’ year of audiology and then COVID hit which fast-tracked me into outreach in Indigenous communities. I went into quite a few communities and spent more than 200 days travelling and working in outback communities.
“There was a lot of paediatric work and otitis media in children. It was an amazing experience and something I’ll never forget, but I got to the point where I wanted to settle down as some months I would be away for two to three weeks at a time.”
Several audiologist friends had moved to Specsavers and after chatting with them, he decided to pursue that option.
“It was enlightening, they were honest and said they really enjoyed the work but it was still hard work,” he recalls. “I think what drew me to Specsavers was the fact I’d have more autonomy but still be working within a framework. I liked the idea I wasn’t necessarily going to be talking to
Images: Specsavers.
Rey Dayap in the Northern Territory Specsavers store where he practises audiology alongside optometrists providing eyecare services.
manufacturers to pick which hearing aids I would be working with because with a franchise arrangement, that’s already sorted.”
Dayap asked a friend to reach out to Specsavers recruitment to see if the network was looking for Darwin audiologists and although it wasn’t advertised, the message came back that recruitment wanted to call him and was keen to talk to him that day.
Soon after, at age 30, Dayap became a Specsavers Audiology partner. He started in September 2023 in an existing Specsavers optometry store within an indoor shopping centre in Palmerston. This location is an added bonus because people walking past with their groceries notice the banner he ordered stating: ‘Audiology now available’.
“I’ve had a great support network. The optometry partner and the retail partner were keen to have audiology on board for some time and it’s been good to have them standing with me. It fosters a good team dynamic and helps the business grow,” he says.
“When customers come in for an eye test if they meet certain criteria, they’re offered a hearing screening by our retail team, and those with hearing loss are offered a chat with me to understand what it means. I can gauge what kind of motivation they have, if they’re interested in a hearing aid, or a chat around communication strategies. If they are interested, I can book them in for a more comprehensive assessment.”
Hearing screening is also education
Dayap says that of those with hearing loss, about half want to discuss it, and out of those, another half are motivated for hearing aids at that time.
“A big part of what I like about Specsavers is how we are educating the public about hearing loss because research shows people often wait up to seven years before acting after finding they have hearing loss,” he adds.
“Having that screening, even if they’re not ready for hearing aids, people start thinking about it and when they come back for an eye test, they might come back earlier for their hearing.”
Dayap has also seen adults with middle ear disease which usually impacts what hearing aid type is best. A device with tubing might be preferable to one with electronic wire which may be prone to more moisture damage, he says. He often refers Indigenous patients over age 50 in this situation to Hearing Australia because it has different funding streams for them. However, quite a few have chosen to stay with him, he adds.
“Specsavers Audiology’s ethos is to provide accessible and affordable hearing care to all and will always provide upfront and transparent information on the best funding options for all patients.” he adds.
Specsavers
provides extensive training
Dayap’s extensive three-week induction covered software, products, training and business skills. Partners can also sign up for other training.
“When the opportunity for my own business came up, I thought, ‘why not?’. Specsavers was very good at making sure you did your due diligence. I was keen to jump on board but there was paperwork and legal documents to read through.”

“I think what drew me to Specsavers was the fact I’d have more autonomy but still be working within a framework. A big part of what I like about Specsavers is how we are educating the public about hearing loss. Having that screening, even if they’re not ready for hearing aids, people start thinking about it.”
Rey Dayap Specsavers Audiology, NT
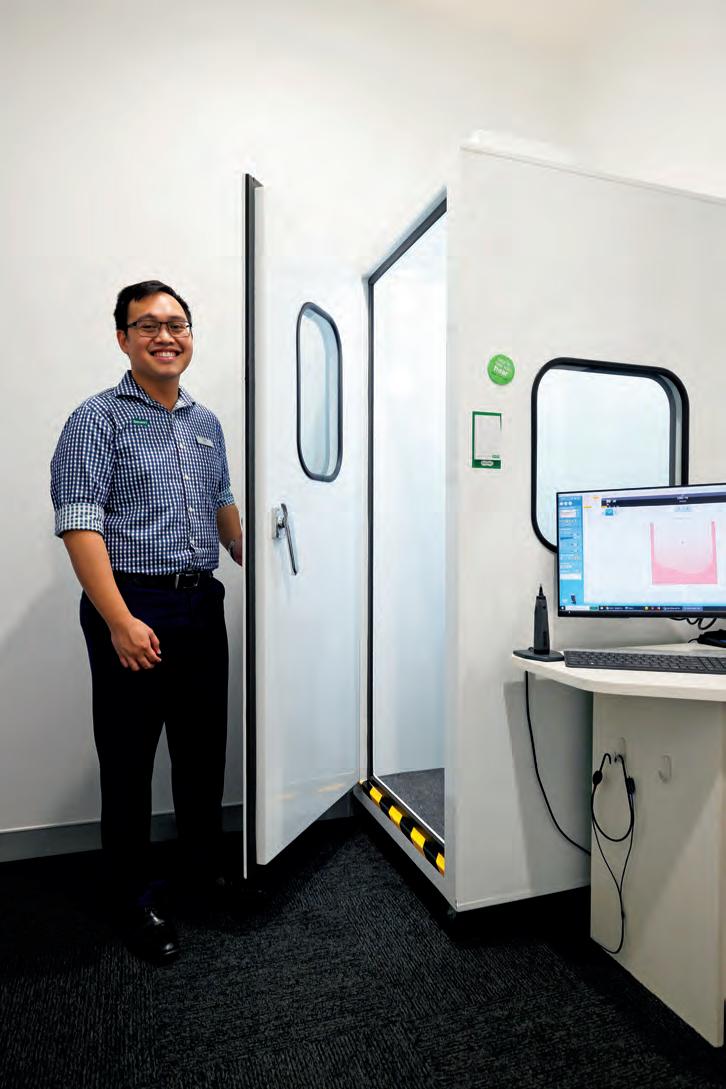
Specsavers set up the clinic. “The optometry team had previously installed a room with a thick door pre-emptively at its last expansion, in preparation for it to be the audiology clinic. Once I was on-board, Specsavers fitted it out with a soundproof booth and provided all the necessary equipment.”
The Darwin lifestyle is another reason Dayap chose to return home. For the first two years he lived with his mother to save rent and whenever he could, he went camping and hiking with friends to the many beautiful national parks in the area.
Reputation helps
He has given hearing awareness talks at Palmerston and Litchfield Seniors Association meetings as the retail and optical partners had a relationship with the association which has already led to increased business.
“The other thing I like is that even though Specsavers has its own brand devices, they’re from three big manufacturers, and within that there is a range of options so I can find something best suited for each customer,” Dayap says.
“People know Specsavers has made a difference for the optical world. People have come in and said, ‘I like what Specsavers has done for glasses and I can see what it’s doing for hearing aids’, and I think that reputation definitely helps.”
One future goal is to work across both existing Specsavers optical stores including the Darwin-based store to extend services to the greater Darwin and NT population, including Katherine, three hours away.
“A lot of Specsavers audiologists work across multiple practices so I’m a bit of an exception but when I signed on that was part of the deal that I would eventually work across both,” he says. “A Hearing Australia team visits Katherine monthly, but I’ve already had patients aware of this who have chosen to travel from Katherine to see me.”
If Dayap’s launch in the territory is anything to go by, things will only get better for Specsavers Audiology and its customers in the top end.
Specsavers fitted out the soundproof booth and provided all the necessary equipment.
Award fit for an audiology king
DR LAURIE UPFOLD, one of the founding fathers of audiology in Australia, received an OAM in the 2024 King’s Birthday Honours list. A living industry treasure, his memory is as sharp as ever at age 90 as he recalls helping to build the profession in Australia.

As one of the nation’s first audiologists, and a founding member of Audiology Australia, Dr Laurie Upfold has lived through decades of hearing advances, was instrumental in developing Australia’s first behind-the-ear hearing aid, trained many audiologists and fitted thousands of people with hearing aids.
But his greatest achievement was during Queensland’s 1963 rubella outbreak when he helped show that babies could be tested for hearing loss and fitted with hearing aids.
Fast forward 61 years and Dr Upfold is walking to the mailbox at his Narrabeen home in NSW. “I found a letter from the Governor General’s office saying I was receiving the Medal of the Order of Australia for service to people who are deaf or hard of hearing. I didn’t believe it! Why should I get such a thing? I was amazed but very proud indeed,” he says.
After graduating from Sydney University’s New England University College in Armidale with a BA majoring in psychology and a history minor, he was employed in 1960 as a psychologist at the government’s Commonwealth Acoustic Laboratories (CAL), now the National Acoustic Laboratories, where he spent the next 30 years.

CAL provided hearing aids for children and deafened war veterans. Dr Upfold knew and understood what the veterans were talking about as he had the same high frequency hearing loss from his shooting history in national service. He saw a variety of deafness problems in veterans including acoustic trauma and middle ear disturbances because the world wars occurred before effective antibiotics and stapedectomy.
“I was fascinated, it was useful work and I enjoyed it immensely,” he says.
As there were no audiologists in Australia, CAL employed psychologists and trained them in audiology. Lead psychologists Dr Brian Harold and Dr Roland Farrant studied audiology overseas and returned to Australia to train him and others.
“There were 12 people doing audiology in Australia in the 1960s, all at the acoustic laboratories, spread over six states,” Dr Upfold recalls.
“I was told training would be ‘on the job’ because there was no university course on the field in Australia, and chief psychologist Dr Farrant was in America doing a PhD in the field, which was called ‘audiology.’ Dr Harold, my supervisor, had completed a PhD at Manchester under Sir Alexander and Lady Irene Ewing, best known for their work testing the hearing of babies.
“I was given a manual, in which was written all that was known about and how to perform hearing tests for adults and children over three, and two
texts, Davis and Silverman’s classic Hearing and Deafness and Ira Hirsh’s Hearing and Hearing Tests. I had an office with a sound-reduced test booth large enough to accommodate a tester, client, parent, desk and equipment.”
After one month’s training he was put to work with repatriation patients and after six months was introduced to school age children then later learnt the Ewing ‘meaningful sounds’ technique for testing babies.
The hearing aid was the Calaid T (for “transistor”), a body level hearing aid in a stainless-steel case in five power levels, with a volume control and induction switch but no tone controls. For every 10 decibels of average hearing loss over 40dB, the aid would move up a step in power which made selection easy, particularly as there was no earmould venting or frequency control variation, he recalls. He also ran lip reading classes to overcome poor speech recognition for people with hearing loss who did not respond well to the Calaid T.
Rubella epidemic
After two years Dr Upfold was promoted to a position in the Queensland laboratory in 1962.
“The rubella outbreak in Queensland in 1963 was Australia’s second biggest epidemic,” he recalls. “We fitted 131 hearing impaired children with maternal rubella histories – one a day for a long time – and there were maybe another 100 with unknown aetiology. It’s no fun to sit and talk to a parent and say your child is never going to speak properly or be in normal education but we were able to help many and provide them with some hope.”
CAL was the state’s only centre for testing babies and young children. “This opened avenues of communication with ENT specialists, deaf schools, paediatricians, speech pathologists and handicapped children’s facilities and led us to begin advocating for early detection of deafness in babies because our work with the rubella children showed it was possible to test babies and fit them with hearing aids,” he says.
“Thus began a career-long interest in rubella, on which I have published
ABOVE, L TO R: The Order of Australia Medal; Dr Laurie Upfold OAM. Image: Laurie Upfold.
several papers, the first in 1970 in the Medical Journal Of Australia in 2004 in the Australian and New Zealand Journal of Audiology."
An ENT surgeon suggested Dr Upfold compile rubella data and publish it in the MJA to urge GPs to refer affected children more quickly for hearing tests. “Some were saying you couldn’t do anything, you can’t test these kids, they’re too young. These deterrents to early diagnosis were problems and that was the point of the articles, to attract the attention of GPs to the problem of German measles in pregnancy,” he recalls.
The strategy worked and more children came forward. It also put the young audiologist on the international map and helped spread the message overseas.
“We were able to make a difference to these kids, particularly those who weren’t totally deaf,” he recalls. “There was a lot of interest in rubella at this time and by the time the Australian babies were one, the Northern Hemisphere epidemic of 1964 was raging and people were looking at what we were saying and doing. A lot of my information was available to them and it was a great help and gave me many overseas contacts.”
Dr Upfold recorded numbers of rubella cases annually and put this information out in various forms including papers on German measles and pregnancy and letters to medical journals in the hope doctors would read them, especially when vaccination was introduced. He remembers one mother of a deaf rubella child who refused to let her other child be vaccinated.

“But vaccination worked, and we never see a rubella deaf child anymore,” he says. “My most important research was on rubella. It was there to support vaccination, attitudes to rubella and its likely sequelae.
“We showed it was possible to diagnose and fit babies and after that, it became standard that babies were fitted with hearing aids, more research occurred in the field and eventually we had a very effective way of testing day old babies. Now every newborn in Australia has a hearing test which is great as we can find them early enough to give them the best possible opportunity in life.”
In 1947, when CAL was established, it fitted veterans and deaf children with hearing aids.
“I’m most proud of the fact I’ve been part of a maturing, thriving profession which is now recognised around the world for its independent research and its service delivery.”
Dr Laurie Upfold OAM, Australian audiology pioneer
“No-where in the world had anything like the problem Australia had because in 1940 the worst rubella epidemic recorded happened here. No-one believed (Sydney ophthalmologist) Sir Norman Gregg when he started saying German measles caused blind babies after hearing two mothers talking in the corridor saying they both had rubella in pregnancy. The world laughed at him but he eventually proved maternal rubella in early pregnancy caused birth defects,” Dr Upfold recalls.
“In the 1940s people believed what happened in pregnancy would not get through to babies and this was the first time anyone recognised that conditions in utero could affect the baby.”
Another advance he was involved with included diagnosing acoustic neuromas. This occurred after publication of a monograph on diagnosis in 1964 and a new surgical treatment of the neuromas involved otologists for the first time, using procedures adapted from the middle ear surgical technique via microscope.
“This was very exciting to otologists, who developed increased awareness of the need for diagnosis,” Dr Upfold says. “A major diagnostic tool was audiometry, particularly the Bekesy audiometer, and CAL had Queensland’s only one, so we saw every acoustic neuroma case from 1962 to 1970 – and I was now a confirmed audiologist.”
Hearing aid revolution
In the mid 1960s a revolution in CAL’s hearing aid work occurred as until then the only hearing aid available was the body-worn Calaid T.
“Suddenly, a new type of aid appeared, an all in-the-ear model called Calaid E,” Dr Upfold says. “By today’s standards, it was awful but back then it really was extraordinary as most hearing aids worldwide were behind-the-ear types, and it was not until about 1972 that Starkey’s marketing brilliance began to make the US market adopt in-the-ear types.
“The E was the leading hearing aid in a government program supplying free hearing aids, not in a commercially dominated market. There was nothing like this anywhere in the world. Calaid E began my love affair with hearing aids which lasted the rest of my career.”
In the 1970s, CAL provided the training course for audiologists in Australia, recruiting 40 or 50 students a year with a psychology background and training them in audiology for a year, but the cost was enormous and some would finish training then quit.
“We had to do something, so we went to the universities and said why don’t you start post-graduate courses in audiology? It’s big-time in America. They saw the point and we guaranteed them jobs against what we knew would be increasing demand; we were sure we could provide jobs if they’d provide graduates,” Dr Upfold says.
Queensland University was the first to take up the offer with a Diploma of Speech Therapy followed by the University of Melbourne’s audiology course instigated by cochlear implant pioneer Professor Graeme Clark who saw the need.
Dr Upfold began working with the universities to develop audiology courses and they were soon under way in all states except Tasmania.
“The profession has grown and grown, and we now have more than 3,600 qualified audiologists as members of Audiology Australia, about 98% of the total practising. I’m very proud of having played a part in doing all this,” he says.
Dr Upfold, a fellow and the first life member of Audiology Australia (AudA), attended all AudA conferences until recently and sponsors the Laurie Upfold prize at AudA conferences for the best paper from a first-year presenter. His ties to the peak body date back to its formation in 1968 as the Audiological Society of Australia, established with 10 founding members, including himself, the councillor for Queensland.
“By this time about 20 people were practising audiology in Australia.
Greg Upfold, Australia’s first second generation audiologist, with his father Dr Laurie Upfold at his 90th birthday celebration this year.
Image: Laurie Upfold.


The Victorian group was meeting once a month talking about the latest papers and got in touch with everyone and said, 'why don't we have a society of audiologists?” he recalls.
Soon after the federal government introduced a scheme for free hearing aids for pensioners to be supplied by the CAL.
“We had the time between the government announcement in 1967 and 1 April 1968 to get ready for the scheme, to get all the hearing aids and staff we needed and train them at CAL in Sydney. It was a big rush job but we trained about 40 people – the equivalent of a two-years Masters course in six months – and it worked well.”
Dr Upfold believes the government was waiting for the Calaid E as such a scheme depended on having a modern on-the-head type hearing aid.
“I was immediately drafted into a position where I worked up many of the administrative details necessary to implement this policy. I’d previously been part of a Health Department team determining the cost of providing hearing aids to CAL’s clients,” he says.
“I became CAL chief psychologist in 1971 and I like to think I gave two significant things to the Australian audiologist: the hearing aid as a significant professional tool, for research and controllable clinical application; and a professional name and definition of the audiologist’s role and work outlook.
“It was apparent to me the future of CAL, and hence Australian audiology, was in the hearing aid but there was little knowledge or research supporting hearing aid activities.”
In the 1960s, there had been only one research innovation, the CROS aid. The CAL course devoted 6% of its time to hearing aids or 8% including ear impression technique, but nothing on acoustics of the hearing aid, Dr Upfold recalls.
ABOVE, L TO R: Beth McLeod and partner Laurie Upfold celebrating his 90th birthday in 2024; Staff of the National Acoustic Laboratories in 1985. Dr Upfold is standing to the left of the woman wearing a red dress in the front.
Developed behind-the-ear hearing aid
The CROS did not use an earmould, which meant its low frequency amplification was reduced, a big advantage, giving the opportunity to make hearing aids more appropriate for not-so-deaf people. Dr Upfold wrote a paper on CROS aids for the Australian Journal of Otolaryngology, pointing out the control it offered to low frequency amplification was its major advantage and this could be tailored using earmoulds with different diameter vents.
He told CAL director, physicist Mr Raymond Piesse, that “we now know something about varying the output conditions of a hearing aid”.
“I recommended we quickly develop a behind-the-ear model hearing aid to take advantage of the venting possibilities and to enable us to use more power in an on-the-head aid. This was the conception of the Calaid H, CAL’s first behind-the-ear aid,” Dr Upfold says.
Colleagues Mr Denis Byrne and Mr Bill Tonisson came up with a selection procedure based on audiometric measurements, not speech, which could be applied to children. It was based on audiometric thresholds and is still the basis of all aid selection procedures. “My task was to implement its use in CAL’s work, and to sell the procedure nationally and internationally. This was a very successful time in my life,” Dr Upfold says.
After three decades with CAL, as administrative tasks grew, he missed practising so quit government work for private practice. He was then a widower, and worked for audiologist Ms Beth McLeod, a widow, in her practice MAC Audiology, now part of the Connect Hearing group, in Sydney. The pair became a couple and the practice is still going, now run by Dr Upfold’s son Greg, Australia's first second-generation audiologist.
In 2008, Dr Upfold wrote
received a PhD from Macquarie University. While practising part time, he wrote the book, a legacy of being a ‘frustrated historian’ from university days. Phonak sponsored it and after the print run finished, leftover copies were given to Australian universities and audiology students.
“I got my PhD 23 years after I got my Masters Honours, a thesis on deaf children and causes, granted in 1985. I enjoyed writing the book and travelling around the country talking to people; it was a good ‘end of professional life’ opportunity. It had to be written and I was probably the best person to do it, especiallly -considering I’d been there while most of it was happening.”
When he looks back on his career Dr Upfold says: “I’m most proud of the fact I’ve been part of a maturing, thriving profession which is now recognised around the world for its independent research and its service delivery. And I’m also proud that my son Greg is the first second-genera tion audiologist in Australia.”


Image: Laurie Upfold.
Image: National Acoustic Laboratories.










More children with moderate to severe hearing loss, rather than just severe to profound deafness, are being implanted with cochlear implants now.

The cochlear implant revolution
The world’s first successful cochlear implant surgery in Melbourne 46 years ago made global headlines and changed the way hearing loss was treated forever. It began a revolution in hearing for severely to profoundly deaf people and it’s estimated more than one million people have since benefitted worldwide. As advances continue to improve outcomes, HPA looks at what’s on the horizon.
As a boy, visionary Melbourne ENT surgeon Professor Graeme Clark, now 89, “wanted to fix ears” because he had a deaf father. His invention became one of the world’s greatest medical research breakthroughs, considered by educators and clinicians to be one of, and possibly the, most important advance in the history of the management of profound deafness.
When he started his research in 1967 on electrical stimulation of the auditory pathways, he did so against opposition from the scientific and medical community. But he persisted and the breakthrough occurred one day at the beach with his children when he examined a Turban seashell and found grass blades would go far enough around the spiral if they were flexible at the tip and stiffer at the base, according to the Graeme Clark Foundation. This mechanical principle was applied to that used for electrodes for the cochlear implant.
After initiating and leading the team that developed the first multi-channel cochlear implant at The University of Melbourne, Prof Clark implanted it in patient Mr Rod Saunders at The Royal Victorian Eye and Ear Hospital in 1978. The Bionics Institute, which he founded to continue development of the implant, states: “Professor Clark knew the operation was a success when his team developed a speech code for electrical stimulation of Saunders’ brain that enabled him to recognise some words without any help from lipreading. Prof Clark says he was so overcome with emotion he went quietly into the next-door lab and cried tears of joy.”
The subsequent Australian-founded company Cochlear established to provide the implants, says when Saunders heard speech, it was the
first time anyone had shown that an artificial sensory stimulus could be interfaced to human consciousness. Prof Clark then became the driving force in seeking government funding for its industrial development.
The multi-channel implant was the first cochlear implant to reliably give speech understanding to severely and profoundly deaf people and spoken language to children born deaf. Improvements made in the years following included a smarter speech code, using implants in each ear to make it easier to localise sound and hear in noise and smaller, safer and more reliable devices.
Preserving residual hearing
The progress continues with one challenge being that the implant can damage residual hearing. Dr Christo Bester, working jointly with the Ear Science Institute Australia and University of Melbourne, specialises in cochlear electrophysiology and cochlear mechanics. He says interfering with a person’s natural level of hearing can limit cochlear implant benefits.
“People with preserved natural hearing tend to do better in complicated hearing tasks that many cochlear implant recipients find difficult – hearing in noisy environments, with multiple talkers, enjoyment of music,” he says.
“Although while 50% to 70% of cochlear implant recipients lose residual hearing, they’re usually already so far down the hearing loss journey that the implant will give them much better outcomes even if they do lose all their natural hearing, they’ll be in a better place,” he says. However, he is working with Cochlear and University of Melbourne cochlear implant surgeons Dr Claire Iseli and Professor Stephen O’Leary at The Eye and Ear to prevent

this happening during surgery and to protect recipients' hearing for the rest of their lives.
Dr Bester has sat in on dozens of cochlear implant surgeries to do this, precisely measuring inner ear function before, during and after implantation. “It’s worth it for memorable moments such as being in the room after we successfully preserve a baby’s hearing during a challenging implantation and being able to say to the parents, ‘Because of what we did today, your child will still have their natural hearing,” he says.
Trauma from the electrode can damage residual hearing as can inflammatory response that damages hair cells, and foreign body response, resulting in scarring.
“During surgery we’re informing the surgeon of changes to the condition of the patient’s hearing by playing the patient sounds and recording the ears’ electrical response to those sounds from the implant as the electrode is being put in. Measuring electrical signals produced by their ear in response to these sounds gives us a way of monitoring the health of the ear during implantation,” Dr Bester says.
“Researchers like me, and a team I’m training, sit at the end of the operating table, watch the condition of the ear and inform the surgeon if there are changes that we associate with loss of residual hearing. If the ear stops responding to us, they can pause insertion and reconsider how far in they’re placing the electrode or alter the trajectory to see if it can be modified to produce best outcomes.
“Our interventional trial at the Eye and Ear basically reversed it and went from 70% of recipients losing residual hearing to 70% having good, functional hearing post implantation”.

Dr Iseli adds: “We utilised this technology to monitor insertion and reduce trauma so we can hear what the inner and outer hair cells are doing while we’re inserting the electrode. This real time feedback has reduced the amount of hearing loss we’re losing and doubled the chance of preserving what natural hearing they have.”
Meanwhile, she says another trial has started at The Eye and Ear and in Sydney and the US of a steroid-impregnated cochlear implant which elutes the steroid post implantation. The hope is this will reduce scarring, foreign body response and inflammation. The Eye and Ear implanted the first patient with the drug-eluting array and has since done two more.
“Similar previous trials involved bulky electrodes and not surprisingly, most people were losing hearing because even if it was preserved in
surgery, they lost it in the first three months because of fibrosis,” Dr Iseli says. “But now that we’re combining the drug with a slimmer electrode, there is potential for the steroids to be hearing preserving and stop swelling, avoiding that secondary loss. It’s a unique opportunity to preserve hearing.”
Robotics is another area of interest. “A steady hand is much kinder on the tissues and no-one’s as steady as a robot,” Dr Iseli says. “In the US they’re doing cochlear implants from start to finish just with a robot but it’s much slower and they were having complications with different anatomies. While that hasn’t taken off, what has is the process of putting the electrode in using a robot and we’ve applied for an insertion robot in Melbourne which is in the process of being approved.”
The robot will be part of Dr Bester’s trial and will be informed by him and his team on insertion so it knows the condition of the ear during cochlear implantation surgery.
“A robot inserts a lot slower than a human; it’s hard to move very slowly to push 22 millimetres in two minutes which is the recommendation,” Dr Iseli says. “The structures are so delicate that the faster you hit them, the more likely they are to be traumatised.”
She predicts the next phase could be gene therapy where implants are an intracochlear delivery method for genetic material to ears that are missing that genetic makeup in people with genetic deafness. “If we became really good at genetic treatment, we might even avoid hearing aids and cochlear implants in people with genetic deafness,” she adds.
Implantable microphone
The microphone remains one of the largest barriers to adopting a fully internalised cochlear implant but US researchers announced in July 2024 that they’d developed an implantable microphone that could lead to fully internal cochlear implants. They claim it performs as well as external hearing aid microphones.
The tiny microphone is a sensor produced from biocompatible piezoelectric material that generates an electric charge when compressed or stretched and measures miniscule movements on the underside of the ear drum. The triangular 3x3mm motion sensor UmboMic comprises two layers of piezoelectric material sandwiched on either side of a flexible
Image: Laurentiu lordache/stock.adobe.com.
Image: MIT researchers and iStock.
BELOW: The UmboMic sensor is a tiny implantable microphone the size of a grain of rice and twice as thick as an average human hair.
Huge improvements in cochlear implant sound processors and their aesthetics, signal processing and fitting software have occurred and will continue.

printed circuit board, forming a microphone the size of a grain of rice and twice as thick as an average human hair.
To maximise performance, the team from MIT, Massachusetts Eye and Ear, Harvard Medical School and Columbia University, developed a low-noise amplifier that enhances the signal while minimising noise from the electronics.
Most fully implantable devices in development sense sound under the skin or motion of middle ear bones but can struggle to capture soft sounds and wide frequencies. UmboMic targets the umbo which vibrates unidirectionally, making it easier to sense simple movements. The goal is to implant it with the cochlear implant and an internalised processor.
Tests in cadaver human ear bones found it had robust performance in the intensity and frequency range of human speech and the microphone and amplifier together had a low noise floor so very quiet sounds could be distinguished. Results showed the necessary broad-band response and low noise needed to act as an acoustic sensor. Researchers are planning animal studies.

“I feel very honoured to receive the award and am pleased the Bionics Institute is expanding our work to other areas,” Prof Clark said. “I am also excited the University of Melbourne has created the Graeme Clark Institute of Biomedical Engineering to integrate research across disciplines to help people with disabilities, and it is good the Graeme Clark Foundation is raising funds to help poor and disadvantaged people in Australia and overseas.”
Bionics Institute CEO Mr Robert Klupacs said the institute’s journey began with development of the cochlear implant which positively impacted the lives of so many people. He thanked Prof Clark for being such an inspiration.
Trials of Cochlear’s totally implantable cochlear implant prototype have occurred at the Eye and Ear, says the hospital’s cochlear implant audiologist Dr Jaime Leigh and it’s likely there’ll be more in future. The version includes an implanted microphone, rechargeable battery and sound processor, as well as an external sound processor which also charges the internal battery. Patients choose between using the external
She says they enjoyed ‘invisible hearing’ – being able to hear without microphone being under the skin which can potentially muffle the signal. Optimising microphone placement and technology is one future design
The hospital has partnered with community audiology providers at 28 Victorian sites involving 36 audiologists to provide services in their local community, training and upskilling them in cochlear implant counselling, protocols and clinical competencies. This model will continue in future and more audiologists will become involved. “The technology will improve, become more automated but how clients apply that is where support from
In Sydney, a trial will test if neurotrophin growth factors inserted during cochlear implant surgery can stimulate auditory nerve fibres in the cochlea
The Cochlear Implant Neurotrophin Gene Therapy Trial will evaluate safety and efficacy of neurotrophin gene therapy after animal studies showed improvement in cochlear implant performance. The fibres grew towards the electrode, “closing the neural gap” and improving the interface between the prosthesis and the cochlear nerve, says the Passe & Williams
Leading the trial are Professor Gary Housley and his team from UNSW, The University of Sydney, The Bionics Institute, Macquarie University, Cochlear and NextSense, whose cochlear implant program medical director Clinical Professor Catherine Birman OAM will conduct the surgery. The trial website says 15 patients will receive the gene therapy and 15 will have standard implants to see if benefits to hearing seen in pre-clinical studies translate to humans. Prof Birman will insert the gene delivery array into the cochlea delivering one drop of DNA solution. A few brief electrical pulses passed between the electrodes will drive the DNA into target cells. Meanwhile, US biotechnology company Sound Pharmaceuticals (SPI) will trial giving its new investigational drug to cochlear implant recipients to see if it prevents and/or treats loss of residual hearing during and after implantation. It received FDA notification in May 2024 that it may proceed with a phase two trial of SPI-1005 (ebselen) anti-inflammatory compound

Image: The Bionics Institute.
Image: Monica Wisniewska/stock.adobe.com.
Thousands more eligible adults could benefit from cochlear implants but only 10-11% are receiving them.



which mimics and induces the activity of Glutahione Peroxidase, an enzyme critical to hearing and balance.
“Ebselen has shown safety and efficacy in three different forms of acquired sensorineural hearing loss in adults including loud sound exposure or acute noise-induced hearing loss, Meniere’s disease, and antibiotic or aminoglycoside induced ototoxicity,” SPI says. The trial with MED EL will enrol 40 adults scheduled to receive a cochlear implant who have moderate to severely impaired residual low frequency hearing at risk of being lost after implantation. They’ll be randomised to six months of oral ebselen or placebo starting two days before surgery.
Lesser hearing loss and more remote fitting
Mr Chris Rehn, chief executive of NextSense, Australia’s largest cochlear implant program with 22 centres nationwide performing around 400 implants annually, says more children with moderate to severe hearing loss rather than just severe to profound deafness are being implanted and he predicts this will increase. Campaigns are also needed to encourage more adults to come forward, he adds.
“We do about 300 implants annually in adults but thousands more could benefit,” he says.
“Our nuture program in the community is one way of introducing the public


to hearing loss so there’s a higher level of consciousness of the need to look at cochlear implants if they’re not getting benefits from hearing aids and it also recommends exploring hearing aids through a hearing aid provider if there’s untreated hearing loss.
“Anecdotally, we’re seeing children with profound hearing loss and cochlear implants do better in outcomes than some kids with lesser hearing loss and hearing aids which challenges us to work out what level of hearing loss works best for a cochlear implant. More cochlear implants are already being done in kids with lesser hearing loss as well as people with single sided deafness,” Rehn says.
“We need to continue building centres where people live. When we opened our Newcastle site we thought we’d get a trickle but we got an avalanche. Removing distance as an impediment to hearing services is important. Manufacturers are also looking at newer and more innovative ways of enhancing technology to interface with people’s complex lives. Already, implants are Bluetooth accessible and work with other assistive listening devices.”
The LOCHI study from Hearing Australia and the National Acoustic Laboratories follows children with hearing impairment and involves NextSense and other organisations.
NextSense head of Cochlear Implant Services, audiologist Ms Eleanor McKendrick, says technology is providing amazing outcomes and proving earlier implantation is better, with the LOCHI study showing babies implanted at six-month-olds achieve better outcomes than later implantation.
“Sound processors worn on the external part of the ear are usually upgraded every five to seven years and that’s where we’re also seeing huge changes in terms of what they can do and aesthetics – they’ve gone from the size of a mobile phone to the size of a hearing aid,” she says.
“Signal processing within the sound processor is always improving and the fitting software is becoming more focussed on remote service delivery so in future, we’ll see more access to remote technology and remote fitting, and remote services will be far more streamlined.”
Dr Leigh, The Eye and Ear’s cochlear implant audiologist, adds it’ll be easier for patients to manipulate their own programs through their mobile phone and while this is happening, it isn’t yet the full suite of services. “They’ll have more control over how their implant and sound processor work and future sound processors will have better aesthetics, be smaller and may proceed to where there’s no visible external or in ear device,” she says.
Dr Iseli concludes: “We now recognise how critical healthy aging is and cochlear implants and hearing aids are going to have an increasing importance and recognition in our ability to keep patients cognitively healthy as well as socially connected so I don’t see cochlear implants going away anytime soon; in fact, I think we’re growing and the future is exciting."
Image: First Voice.
Children with cochlear implants (from left) Billy, Charlotte, Emily, Henry, Tim and Kyden, recently spoke at First Voice’s Power of Speech event at Parliament House.
ABOVE, L TO R: Dr Christo Bester from Ear Science Institute Australia; The Royal Victorian Eye and Ear Hospital cochlear implant surgeon Dr Claire Iseli; The Royal Victorian Eye and Ear Hospital cochlear implant audiologist Dr Jaime Leigh; NextSense chief executive Chris Rehn; NextSense head of Cochlear Implant Services audiologist Eleanor McKendrick.
Cochlear’s Nucleus

Cochlear’s SmartNav a smart move
For the first time, surgeons performing cochlear implants have access to a navigation tool that provides live insights during electrode insertion and final placement. Benefits include confirming that the electrode is in the correct final position immediately upon insertion, preventing the wait for imaging post insertion to confirm correct placement.
Cochlear’s Nucleus SmartNav System has only been on the Australian market since June 2023, yet it is already in use in nearly half the hospitals that perform cochlear implants.
Leading cochlear implant surgeons Professor Robert Briggs and Dr Benjamin Wei from Melbourne, featured at right, are among surgeons providing excellent early feedback on the intraoperative tool that gives real time information during surgery for in-theatre decision-making around angular depth and speed of electrode insertion.
The system includes an iPad app, which visually gives a representation of what happens as the electrode is inserted, and a surgical processor. It provides diagnostic measurements to confirm integrity which Cochlear says can improve surgical consistency, facilitate optimised electrode positioning and increase surgical confidence. It also means electrode irregularities can be detected and corrected during surgery.
Mr Nicholas Guildhary, a Cochlear audiologist rolling out the SmartNav across Asia-Pacific, says its controlled market release data on 119 surgeries in North America and Europe reveals 97% of surgeons using the system say it reduces complexity in surgery and has a positive impact on their surgical process.

“There are pre-operative tools that help surgeons plan cochlear implant surgery but this is the first tool to show what’s happening in surgery and give a live diagnostic,” Guildhary says. “It’s unique, having that real-time diagnostic for Cochlear Nucleus implants, which comprise most of our implants.”
Cochlear says traditionally surgeons rely on surgical skill and a steady hand to insert the electrode array but SmartNav provides unblinded insight during insertion. If an issue is identified, they can address it immediately.
The implant directly stimulates the cochlear nerve so signals are sent to the brain and interpreted as sound but sub-optimal electrode placement can affect this. With final electrode placement correlating with hearing outcomes, it’s important to have reassurance and confirmation the electrode is placed properly and performing as intended, Cochlear says.
The technology enables the surgeon to see if the electrode is performing and test how the nerve is responding to the electrode during insertion.
“SmartNav is a convenient, effective and easy method of checking that the electrode is working, that the nerve is responding as we expect, and it tells us the electrode is in the right position.”
Professor Robert Briggs Cochlear implant surgeon
Generally, surgeons confirm electrode placement via X-ray imaging in the operating room or post-surgery but this is based on imaging availability and some hospitals may not have immediate access. The system also gives surgeons the ability to compare how steady their insertion is over time. Cochlear says wireless connectivity and intuitive design deliver a seamless workflow through the iPad. The surgeon views details including:
• Placement check which gives information on final electrode placement and is designed to reduce the need for intraoperative imaging post electrode insertion.
• S peed of insertion which provides feedback on speed and consistency of electrode insertion.
• Impedance which provides assurance the device is operating as intended before leaving theatre.
• Advanced and AutoNRT measurements for obtaining neural response telemetry thresholds, providing flexibility in settings for optimal measurement.
• Electrical Stapedius Re ex Threshold (eSRT) to confirm nerve response to electrical stimulation to establish stimulation thresholds.
Audiologist mapping benefit
Another benefit is that intraoperative data is securely imported into Custom Sound Pro fitting software at the recipient’s fitting clinic to inform audiologist
Images: Cochlear.
SmartNav System has many features to help surgeons with final electrode placement.
Image: Cochlear.-
mapping of the sound processor, contributing to efficient post-operative management. Currently data is sent to audiologists in paper versions.
“Compared to the current state, there’s no way to easily send data from the theatre to the clinic where the recipient will have their sound processor switched on. Through secure cloud or email transfer, data collected during surgery through SmartNav can be seamlessly transferred with the click of a button to the fitting clinic and used to do the initial activation with the sound processor,” Guildhary says. “Anything that better informs the audiologist of what’s happened in surgery helps because it might influence how they program the implant.”
Several studies including multicentre studies of about 500 cases have compared SmartNav surgeries with standard surgeries with results expected to be published soon.
The system also won gold in 2022 in the Australian Good Design Awards’ medical and scientific product category.
Highly recommended by surgeons
One of Australia’s most experienced cochlear implant surgeons, Professor Robert Briggs, says it’s a convenient and effective way of checking that the electrode is working and the ‘placement check’ feature confirms the electrode is in the correct final position.
Prof Briggs has been doing cochlear implant surgery for more than 30 years and has performed more than 1,000 procedures.
The University of Melbourne Clinical Professor operates at The Royal Victorian Eye and Ear Hospital and the Royal Children’s Hospital, as well as St Vincent’s Private Hospital. He has been using the SmartNav routinely during surgery at The Eye and Ear and St Vincent’s over the past six to 12 months.
“It’s a new system to assist with intraoperative and early post-operative testing of the implant,” he explains. “I knew it was being developed by Cochlear and we were keen to be involved in using it and testing it out.
“It allows testing of the implant function and helps position the electrode inside the inner ear. It measures responses from the nerve at the time of the operation and is a convenient, effective and easy method of checking that the electrode is working, that the nerve is responding as we expect and it tells us that the electrode is in the right position.”
Surgeons could not previously tell if an electrode might fold on itself, creating a problem inside the inner ear, Prof Briggs adds.
“We used to rely solely on an X-ray after insertion to check this but SmartNav has given an additional measurement of helping confirm (if an electrode is folding). There have been cases where the placement check shows the electrode has possibly got a fold in the top of it which means it can be removed, replaced immediately and checked again to ensure it has not folded and is in the correct place. This is a major advantage.
“If the electrode doesn’t go in as far as it should, it won’t give the same degree of electrical stimulation benefit. A fold is relatively uncommon but it’s very important to recognise if it does happen because it can then be corrected immediately. It’s better to recognise at the time of insertion rather than post-operatively with X-ray because if not recognised initially it needs a separate operation to fix it.”
Prof Briggs says imaging is still done at the same time or immediately after the insertion or post-surgery as a double check to ensure the electrode is in the expected position. He says the system’s speed of insertion feature may “help with hearing preservation”, in future.
“It’s better for the surgeon and the patient," Prof Briggs adds. “It’s an elegant system and I’m sure Cochlear will continue to refine it and develop more things in terms of telling where the electrode is inside the ear which will become more helpful. We recommend all surgeons in Victoria use it; this is already happening in our clinics and I know they’re keen to continue. Undoubtedly it will be increasingly widely used around Australia as it’s a worthwhile system.”
Dr Benjamin Wei, cochlear implant surgeon at St Vincent's Private Hospital, Melbourne and The Royal Victorian Eye end Ear Hospital.


Improves surgery efficiency and assesses implant integrity
Also praising the system is ENT surgeon Dr Benjamin Wei who also operates at St Vincent’s Private Hospital and The Eye and Ear in Melbourne. He has been performing cochlear implantation for 14 years and has used it in more than 30 cochlear implant surgeries since 2023. Dr Wei says he is impressed with how it improves the efficiency of surgery.
“The real time feedback of the insertion process including speed, depth and angle provides extra information to help surgeons achieve a better placement of the electrode and also provides reassurance that the electrode is functioning satisfactorily,” he says. “In terms of technology it’s one of the biggest advances in the assessment of the implant integrity as it confirms the correct placement of the implant. It has really changed the management and is more user friendly and efficient. I highly recommend SmartNav. It’s one of the extra tools that can provide surgeons additional information which makes the surgery more efficient.”
Dr Wei says it also reduces theatre time which is important for children and elderly patients under general anaesthesia and is helpful in multiple cases, due to reducing the time required to perform integrity testing of the implant during surgery. However, imaging is still routinely performed at the same time or immediately after the insertion or a post-surgery CT scan double checks and confirms the electrode is in the expected position.
“Sometimes the nurse tells us the iPad reading but I also use the voice activation setting so I can hear how deep it is in the cochlea without having to look at the iPad,” he says. In future, this information could also prove valuable for research particularly around the speed of insertion and placement in terms of trauma, he adds.
The system is on an iPad so it is light and easy to use.
Image: Dr -Benjamin Wei

Making a statement
DEAN LAIRD has worked in the hearing industry for nearly four decades but believes his latest project is one of his most important; reducing stigma through beautiful and functional jewellery and accessories for hearing aids and cochlear implants.
Adelaide audiometrist Mr Dean Laird is on a mission to accessorise hearing devices, which in turn reduces stigma for children and adults. The stunning Deafmetal statement pieces he sells enable people to transform the look of their hearing aids and cochlear implants into personalised jewellery and allow them to be secured with style.
Glasses are now fashion statements, with stylish, designer pieces reducing stigma around wearing spectacles to correct vision.
Laird wants the same principles to apply for hearing aids, cochlear implants and bone-conduction device headpieces, so those with hearing loss can feel empowered and not embarrassed by their condition or the assists they use to aid communication.

The journey began three years ago when he stumbled across a LinkedIn post about Deafmetal jewellery and accessories for hearing devices designed and created by Finnish fashion designer Ms Jenni Ahtiainen after she developed hearing loss in 2018.
The post was by an American audiologist who had taken up distributorship of Deafmetal in the US. He contacted her and she put him in touch with Ahtiainen in Finland and from there, he became the Australian and New Zealand distributor.
The Finnish designer says, on her website https://deafmetalau.com/:
“In 2018 when I got my hearing aids, I put them behind my ears and started to think. First, I innovated a small holster you adjust around the hearing aid and into the holster I added some leather strips and suddenly the hearing aids looked like me, they felt more like me and I looked like me, so Deafmetal was born by the hands of a hard of hearing designer.”
The main innovation – the flexible holster – is the linchpin and insulates dampness or sweat absorbing into the battery locks. It attaches to behind-the-ear hearing aids and cochlear implants. Earring chains, safety rings and other designs are attached into the holster.
“Deafmetal makes your hearing aids look like jewellery so it decreases stigma experienced my many hearing aid users and it looks like normal jewellery but the earring chains are also safety chains to stop hearing aids falling out,” she adds.
Rings that clip onto the ear and hearing-aids through the holster also stop hearing-aids falling out.
“The mission is to change the thinking, so that hopefully in a few years it will be common for hearing aids to have adornments, we’re not worried about them being seen, in fact they are celebrated.”
Reducing stigma and celebrating hearing aids
Laird, who has worked in the sector for 36 years and owns My Hearing clinics in South Australia, says he has always looked for new ideas and innovations in the hearing sphere.
“I’ve worked in various positions, have sold a business, worked in vertically integrated operations and for hearing aid manufacturers and done the full circle back to independent business again,” he recalls.
“What really resonated with me was that being a hands-on clinician for 80% of my career, stigma around hearing loss has been there all the time. It's what everyone talks about and says if we could get rid of stigma, why wouldn't we? How do we do it? It's brought up in every conference I’ve attended.”
Ahtiainen says in a video on the website: “Why is it that people can get glasses to fit their style and personality yet hearing aids don’t individualise people? This is one way that people can be themselves, add on and be more proactive about being proud, not hiding that they've got a hearing problem.”
Laird adds: “It shows their personality and how they want to dress up their hearing aids. The mission is to change the thinking, I guess, so that hopefully in a few years it will be common for hearing aids to have adornments, we’re not worried about them being seen, in fact they are celebrated.”
Although products are high quality and European design, prices are reasonable for a reason.
“We want them to be accessible to everyone and don’t want to discriminate against anyone. It’s not about money, this isn’t about making a profit but it’s part of the journey of being in the industry. I'm 57 and maybe in 20 years, this sort of thing might be more common and viewed as a fashion statement like eyewear,” Laird says.
The designs started with a women’s range of earrings for hearing aids,

Images: Deafmetal.
Dean Laird Deafmetal ANZ
Kids love the fun cochlear implant transmitter coil covers or 'cochlear hats' which come in a range of styles and colours.
and cochlear implant transmitter coil covers or ‘hats’ for children followed by a men’s range which includes darker, thicker rings that look more modern and tougher. Collections evolve as fashion and style changes.
To spread the word, Laird has shown the products at conferences including ACAud inc HAASA and Audiology Australia events and marketed the product to the profession in New Zealand. Various audiologists have stocked them in Australia and supporters include NextSense, but sales of the products are mainly online.
Making people feel good about themselves
Best sellers include safety rings that clip on the pinna near the top of the ear as they don’t need a piercing, are unisex and help hold the hearing aid in place so it isn’t flicked off or becomes lost with masks or jumpers coming off. Silver chains that click to the back of the hearing aid on the holster and attach to a stud or combine with a stud are also popular.
“At some schools children can’t wear jewellery but it’s almost like kids with hearing aids and cochlear implants can get away with more because they can wear the jewellery and say it’s to help them not lose their hearing aids. It flips it on the head because instead of being singled out for their hearing aids they’re allowed to be cool, wearing jewellery,” Laird says.
“They can have many designs or for the cochlear hats which stick on the transmitter with velcro, there are unicorns, colourful puppies, or Pow! covers which make them feel important. I’ve had so much good feedback from people, even hearing professionals for instance who’ve lost hearing and they think it’s amazing to be able to put something on themselves and feel good about themselves and look good, so it's a no-brainer. You wonder why it hasn’t been done before.”

Testimonials from happy customers are on the website. Laird’s son Rory plays for the Australian Football League team the Adelaide Crows, and another idea he’s considering is football covers or stickers for cochlear implant caps and headbands. Laird adds: “It’s fantastic to help people with their hearing. That's why we exist and we get a thrill out of that and satisfaction that we're helping people. But it's also enlightening to get responses from people saying this is what’s been missing. This is a missing link where the hearing impaired can be themselves and help to reduce any stigma associated with a hearing device. For first time users and kids, it makes them more comfortable and confident. It’s that simple! “Nowadays, every second person's got something hanging off their ear whether it’s an ear-bud or an earpiece for their phone so let’s celebrate it like we do with vision and glasses and make it normal and accepted."

A shield of courage
Indigenous deaf artist and LGBTQI Gadigal and Wonnarua man Mr Daniel McDonald is the talent behind the striking Shield artwork, on the cover of our magazine, that brought an Australian flavour to Deafmetal

McDonald has exhibited his vibrant dot paintings in Australia and Japan through his business Deadly Hand Talk (deadlyhandtalk.com).
‘Deadly’ is Indigenous slang for proud or awesome while ‘hand talk’ means communication by hand.
Mr Dean Laird recalls: “I was looking for an Indigenous influence to make some of the jewellery Australian and one day I was watching TV and saw Daniel. The show mentioned he was hearing-impaired so I approached him about using his stunning art on the cochlear hats.”
A partnership enabled Deafmetal to turn Shield into a cochlear implant transmitter coil cover and Laird says it has driven a lot of interest. McDonald says: “Shield is a good word for our community. The U shape means person and ‘l’ means spear. The circle means campsite for all different diversity of LGBTIQ and others. The artwork uses some Indigenous symbols for protection and has LGBT colours. I hope it works as a match with cochlear implants. I want to help people to overcome their barriers and to never give up.
“When I put the shield on and walk out with it, people look at my shield cochlear implant and ask me where I got it from. I have shown people the Deafmetal website. It made me happy that they know I have a cochlear implant with my artwork on it. I am proud of it. It helps people to see and know that I am hearing-impaired and they won't ask me because it stands out and makes a point. It is a great idea for the future from Deafmetal; they can make cochlear implant covers to suit different kinds
Deaf Indigenous artist Daniel McDonald, the man behind the Shield cochlear coil hat.
Image: Daniel McDonald.
The men's range is a recent addition which is also proving popular.
The hearing aid jewellery and accessories are functional and stylish.
The beautiful ear-rings double as a safety chain for hearing aids.
Helping people escape auditory processing disorder
Ex-patriate American audiologist DR ANGELA LOUCKS ALEXANDER lives on Queensland’s Sunshine Coast. She has overcome abuse to shine on the world stage and establish the Auditory Processing Institute to train her peers and help patients escape "the hidden prison" of APD.

After working with auditory processing disorder (APD) patients for two decades, Dr Angela Alexander is on a mission to put the condition on the map and train audiologists worldwide in effective diagnosis and treatment. She is so passionate about spreading the word that she even hosted a TEDx talk featuring a harrowing recount of her childhood, which was the most watched TEDx worldwide in September 2021, attracting 1.1 million views.
Her message is simple: it’s vital parents, teachers, health professionals and people with this often-neglected disorder know it is real and something can be done to help the many people it is preventing from living a full life. She has even successfully treated many colleagues and other health professionals who were both previously unaware of the impacts of APD.
Prevalence estimates vary from 3% to 10% of the population, meaning up to 2.6 million Australians could be affected. APD is a generic term
for hearing disorders that result from atypical processing of auditory information in the brain and relates to how efficiently and effectively people process what they hear. The ears and brain don't fully coordinate to understand sound, especially speech.
“Most people affected by APD don’t even know it exists and most health professionals who know it exists don’t realise it can be treated beyond devices. I’m working to change that by training audiologists how to identify and treat it through my institute,” she says.
Dr Alexander has evaluated and provided therapy to hundreds of patients so they can hear and understand more quickly and accurately. In the past six years alone, through her institute, she has upskilled about 250 audiologists and speech pathologists globally in diagnosis and therapeutic options; about 80% are from America and Canada, 10% Australia and 10% other countries. “It’s exciting because when I started there were maybe 250 people treating APD worldwide so we’ve about doubled it but there is still such a long way to go,” she says.
Does the patient say they have difficulties?
The institute stemmed from a lifestyle change when Dr Alexander had her daughter in 2018 while living in New Zealand and working in her private practice seeing APD patients full-time.
“I was most of the way through my pregnancy with Isobel when I realised my therapy clients weren’t going to have any help,” she recalls. “I thought, ‘I think I can make a therapy program online that they can follow’, so I created a direct-to-client program.
“Then an audiologist reached out and asked, ‘if you can treat someone online, could I take that and learn how to do the treatment?’ That started my first course in auditory training. Then someone else asked if I could teach diagnosis too. I took that as a sign to get started.”
In 2020 after living in New Zealand for 10 years, she moved to Australia with her family during the pandemic. Lockdowns meant audiologists had time at home and the online courses took off. “There was a growing contingent of hard-working, creative audiologists wanting to learn how to do this work in their private practice. I led courses over Zoom and through on-demand lectures, and switched to tele-practice for my patients,” she recalls.
“I believe every dispensing audiologist should have APD assessment skills because once you start sensing these red flags you should be able to help patients. Everyone with APD can have some type of improvement with auditory training. We need to identify them and realise there are treatments available and we need to do this more proactively.”
APD is not on the curriculum at all universities, Dr Alexander says. “Audiology hasn’t done a great job of working together on this project and that's one thing I am trying to change. The most important part is, ‘does a patient say they have difficulties?’ In audiology we are so used to saying, ‘I'm going to do this test to tell you if you have a problem.’ We need to look at it the other way around; does the client say they have a problem? If so, we need to use tests that quantify that problem and devise a treatment plan and we haven't been doing that well.”
Dr Jack Katz, a world-leading expert in APD therapy from the US,
Images: Angela Alexander.
Audiologist and TedX speaker Dr Angela Alexander established the Auditory Processing Institute.
describes it as, “Auditory processing is what the brain does with what the ears hear.” Dr Alexander expands on this saying, “auditory processing is the function and APD is when that doesn't go well and it could happen anywhere along the auditory pathway.”
Causes could be congenital, acquired from middle ear infections, head injuries or demyelinating disorders. “I see families whose entire family has struggled with this for potentially generations,” she says. Up to 50% of adults with ADHD and half of adults with developmental dyslexia may also have auditory processing issues and there is also crossover with autism, she adds.
Locked in the basement
In her TEDx talk, she tells her horrific story of growing up in America and being locked in the basement by her father and step-mother from age 13 to 17, only allowed out to attend school as punishment for “not being able to focus”. Frightened and ashamed, she was told she was dumb and not smart enough for university.
“I tell my story because I know what it feels like to be set aside, to be dismissed, to be imprisoned and I also know how it feels to be set free,” she says. Her story of entrapment mirrors that of the patient being imprisoned by APD and set free with treatment.
“The academic issues I had growing up, listening difficulties, trouble following instructions, I looked like I was not paying attention but I was overwhelmed trying to listen. I remember feeling lost and confused, something I often see in my paediatric patients," Dr Alexander recalls.
“Although I have never been formally assessed for APD myself, I believe my difficulties understanding what I heard put barriers in front of my learning but I loved school, I loved the times when I was out of the basement; that was the best ever, I was upstairs and I wasn’t alone.”
After being rescued by a group of brave girls and strong women from her school, and a kind foster mum who reconnected her with her mother, she blossomed personally and academically. However, at university, she often fell asleep in lectures, tired from listening, and had to record lessons and listen three times to understand. Then, 20 years ago, in April 2004, while finishing her Bachelor’s degree in speech pathology, Dr Katz delivered a lecture on APD and changed her life. She felt like she was learning something she’d already known.
“That's when I decided, this is what I’m going to do,” she recalls. “I walked up to Jack and said, ‘I’ve got to see how you test for and treat it; I need to see it with my own two eyes.’ He said to go to his clinic next week for an hour so I went and watched him then asked if I could return next week, and it continued.”
She worked with Dr Katz from 2004 to 2012, building knowledge and expertise in APD, while graduating from the University of Kansas with a Doctor of Audiology. After observing him providing treatment, she could understand lectures immediately. “I didn’t realise APD had affected my own life until it was resolved,” she says.
“Jack’s now 90, and we’re still working together online for adult clients

“Most people affected by APD don’t even know it exists, and most health professionals who know it exists don’t realise it can be treated beyond devices. I’m working to change that by training audiologists how to identify and treat it through my institute.”
Dr Angela Alexander Auditory Processing Institute
Dr Alexander using a visual filter to cover her mouth during auditory training sessions. This helps the patient focus on auditory input.

with auditory brainstem implants. (ABIs). Only 10% of people with ABIs have open-set word recognition and can understand speech in quiet but so far, all three of ours have.”
Dr Alexander says there is potential for auditory training to extend to hearing aid users and ‘brain fog’ patients, as her research suggests post COVID-19 brain fog could be related to APD. She has, however, had a few clients for whom the therapy did not provide substantial benefit but these were largely clients not engaged in the process, she says.
She has done auditory training at her daughter’s primary school, deemed ‘listening lessons’ that helped children improve auditory skills and taught teachers how to recognise APD. “An audiologist in her 60s came up to me after a presentation and said she didn't know we could treat APD, which she reported having had all her life, so I treated her and she had amazing results. There are so many more people we could help,” she says. Another case, an American doctor who reported COVID brain fog, saw ENT surgeons and audiologists but was told to meditate and ‘listen harder’. His mental health was suffering but he found it mind-blowing when he was finally diagnosed and treated for APD.
“APD is the ADHD of the future; years ago, ADHD was not talked about, and people thought not much could be done. Now, this is in that sphere,” she adds. “With APD, the clinician often has the denial, not the client; the patient want answers and are disappointed when the audiologist says there’s nothing wrong with their hearing. So it's refreshing for an audiologist to hear from a client, ‘I have problems. I want to do something about this’.”
The institute has courses to train audiologists and speech therapists in APD diagnosis and treatment and a map to locate practitioners and online auditory training for patients. The apdsupport.com website has free resources including letters to give teachers, coaches, parents, and employers which explain APD and give tips as having supportive and understanding people around them is life-changing.
“There was a misunderstanding in audiology that there weren’t tests to assess auditory processing in children under seven but there are many tools now for children aged four and older. We have tools to measure auditory skills in infants and a new ‘Frequency Following Response’ protocol from Dr Nina Kraus can measure auditory processing abilities in infants. Early intervention is so important. To quote speech pathologist Maryann Kaminsky, ‘If we know that auditory skills underpin early literacy, and if we want all children to read by seven years of age, why would we wait until then to assess them?” Dr Alexander says.

Raising the bar in community and GP education
A Better Ear independent audiology practice near Brisbane is owned and run by audiologist PENELOPE WOODS and her husband DAMIEN WOODS, the clinic’s business manager. They explain how their education-based approach is leading to a successful enterprise.
Educating their patients, the community and GPs about hearing loss is the ethos of A Better Ear and it has worked wonders for the business. In just over five years, and despite the COVID-19 pandemic hitting them one year in, Penelope and Damien Woods have built a thriving independent practice that serves the coastal city of Redlands, which is about 25 kilometres from Brisbane.
Penelope, the principal audiologist, and Ms Amanda Ariotti, clinical rehabilitation audiologist, pride themselves on educating patients at the clinic and in the community through regular speaking gigs and a column in the local newspaper under the banner, ‘healthy hearing for a healthy life’.
GP visits to advise and update doctors on the latest hearing evidence also form a vital part of their education strategy. In fact, referrals from GPs that stemmed from these visits helped keep the practice afloat during lockdowns from the pandemic.
“In February 2020, one year after we started, we had our best month ever then COVID hit in March 2020 and we were 95% down on the previous month,” Penelope recalls.
“Pretty much straight after we opened in 2019 we started visiting every GP clinic in the Redlands that would have us which is super important because I've been told by GPs they only have 30 minutes of audiology in their entire medical training so some of the things I talk about with them are a surprise.
“It's important for them to know about the hearing system, things they need to be aware of that might be a medical emergency, and looking out for older Australians so they can hear well and lead a rich, fulfilling life. Being socially connected is more important than not smoking or drinking for mortality and morbidity and it’s vital they understand that link.”
Penelope estimates that she’s spoken with about 100 GPs, typically as a group at general practices during lunch.
“I’ve done a lot of tinnitus training and will take on complex cases so it’s a relief for doctors who often don’t know where to send these patients,” Penelope adds. “Another time we visited a surgery with a great bunch of engaged, proactive doctors including one who specialised in dementia.
“She had been administering a verbal questionnaire testing cognition but never thought to look in patients’ ears first. We advised if doing verbal questionnaires to assess cognition you should first check they can hear you.
After our talk the practice updated its protocols and added a hearing check to this and annual patient testing.”
Annual GP visits and interesting cases
The audiologists see each GP they have an ongoing relationship with once a year to bring them up to date on latest advances.
Damien, who is the clinic’s business manager and a talented illustrator, is a business and marketing specialist who previously led teams at The CEO Institute and Vita Group Limited.
He says that as a result of the ongoing relationships with GPs, the clinic has strong referral relationships with the doctors and receives a varied and interesting caseload.
"If you’re an audiologist, you might not initially think about talking to your local GP. However, by collaborating with local doctors, you'll likely encounter a variety of cases such as tinnitus, exostosis, and middle ear pathologies,” he says. “This collaboration not only brings in more diverse and interesting cases but also serves as professional development. Your understanding of various medical conditions and treatments will improve, making you a better and more integrated audiologist within the community you serve."
A Bettter Ear also gives presentations at community groups and service clubs such as Rotary, Probus and lawn bowls clubs at least monthly and sometimes twice monthly.
“It’s about delivering evidence-based information in a way that’s easy to understand and highly engaging. People always respond well,” Penelope says. “We mention a bit about ourselves, we make sure we’ve got a really good presentation and PowerPoint, keeping it relevant, interesting and project our voices which is easy for me because I was a singer. If you are a bit timid, just practise, practise and more practise.”
Damien does research beforehand, contacting groups and teeing up dates. They have even booked spots for next year already. Patients also often suggest the audiologists give a hearing health talk at their clubs and provide contacts.
Be closer to your community
The fortnightly newspaper column they write helps the public learn about hearing and gives them exposure as ‘your local audiologist’.
Images: A Better Ear.
Penelope and Damien Woods are partners in life and their audiology practice, A Better Ear.
“I've been told by GPs they only have 30 minutes of audiology in their entire medical training so some of the things I talk about with them are a surprise. I’ve done a lot of tinnitus training and will take on complex cases so it’s a relief for doctors who often don’t know where to send these patients.”
Penelope Woods A Better Ear

doing, and feel strongly that we're doing good work.”
Their love for their work shows as does the community appreciation. Photos of Penelope with smiling patients presenting flowers, chocolates and thank you cards on their website and five-star Google reviews are something the couple is proud of and has worked hard for.
“When people are in here, they're always saying, ‘Wow, that was the most information that I've ever had’, or ‘that was so educational and worthwhile, no-one's ever explained it like that’,” Penelope says. “They’re so grateful that you’re taking care of them and are interested in them. I always say it’s their body and it’s important they understand how their body is working so they can make an informed decision. Our job is to educate and assist them.”
Damien says it’s important to be authentic and non-transactional; they’re interested in long term relationships and avoid rushing appointments.
“We moved to larger premises in February in a medical precinct with better appointed rooms, and we have nice couches in the reception area, plants, and no merchandise or posters from manufacturers because we are about hearing care, audiology, and the devices come after that,” he says.
“It starts when people walk in by getting their blood pressure to drop. We use a signature scent so it's all about getting people to come down to that comfortable state.”
Benefits of a business manager
While some husband-and-wife teams might find working together challenging, Penelope says having a business manager is a gamechanger and Damien is perfect for the job.
“None of this would be real without Damien's expertise, his analytical, planning and business skills. He keeps me organised so I can do the rich work that I do,” she says.
Her husband adds: “We’re very different, but that makes us complementary. My job is to provide a foundation that allows Penelope to realise her vision. Operationally, I've not lived and breathed audiology prior to this so we're able to think more creatively about the way we deliver value.”
The first 3.5 years it was just the two of them, but they have now expanded the audiology team and front of house staff. They wanted autonomy to choose the hearing aid that best suits each patient rather than being bound to certain manufacturers.
Penelope has her top four that she prefers based on product quality and after sales service.
“Our brand was more focussed on being a “fair price option” when we started but we now focus entirely on “patient-centricity” and reliable hearing rehabilitation. Balancing those visions and managing our brand and communication is where I come in as the business manager,’” Damien says.
Penelope adds: “We're always thinking about how we position our audiologists as being what you're paying for. A lot of patients ask you to help find the best product but all that we offer are excellent, we're spoiled for choice. There are clinical considerations for each patient that make this one more appropriate than another.
“People with hearing loss generally have a poor understanding of the factors that determine success in hearing rehabilitation. We try to improve that situation through an educational treatment model. Device choice is important but not critical but best practice audiology is not optional and we believe that practising the best audiology is the right thing for our patients and for our business.”
Penelope initially did an undergraduate degree in vocals and music at Queensland Conservatorium.
“Musicians have different expectations from their hearing than non-musicians, Damien says. “We understand those expectations because both Penelope and I are musicians. Best practice audiology is still best practice but to be truly focussed on patient need it is sometimes helpful to additionally use sounds they want to hear a certain way. Obviously tuning a hearing instrument to a cello or clarinet is different from tuning it for speech.”
Penelope was a mature age student in her 30s when she enrolled in her Masters of Audiology in 2014 as she waited until their daughter was in school so she could study full-time. Ten years later, everything has come full circle, with a well-established career she loves, a practice she enjoys working in with her husband, and a business that gives back to the community.

Penelope Woods giving one of her many community talks, educating groups of people about hearing health.
The frontier of Ménière's disease
World leading Ménière's disease researcher PROF JOSE ANTONIO LOPEZ-ESCAMEZ moved from Spain to the University of Sydney to establish the Ménière-Neuroscience Laboratory at the Kolling Institute, Sydney. He discusses genetics of the disease, planned gene therapy trials and establishment of a global database along with tips on treating Ménière's.

While doing hospital rounds in Spain, ENT surgeon and neuroscientist Professor Jose Antonio Lopez-Escamez noticed Ménière's disease was almost a neglected condition. This is when he decided to dedicate his career to studying the disease, working to uncover its causes and give patients viable options for relief and even cure.
“When I started practising, most of my patients had benign paroxysmal positional vertigo and many had severe Ménière's with bilateral hearing loss that started in their 30s,” he recalls. “These patients were in very poor condition. Nobody knew much about the aetiology and no-one was very interested in them because there was not really any research or effective treatment, so they were kind of ignored.
“I began seeing these patients and collecting clinical information. We identified different clinical subgroups including those with a family history of the condition. One main finding is to look at the history of hearing loss or vertigo in their parents or other relatives. Some have incomplete forms of the disease, for example just with hearing loss.”
Prof Lopez-Escamez says that estimates of around 10% having a family history of the condition are probably an underestimate. These data are from Europe, and the disease seems to be less common in East Asia.
“We found most patients with Ménière's had a recessive inheritance, and their doctors were not aware it was a genetic condition. If you ask the patient, they will tell you that nobody in the family has MD. Many of these patients have a recessive disease, meaning they have the disease but their parents are only carriers of one of the alleles and both parents are healthy,” he explains.
“We found the most common gene in familiar cases shows a compound recessive inheritance pattern, meaning that they have one mutated allele from the mother and a second from the father and you need to carry two different mutations to develop the disease. This is what we found for a gene called OTOG that encodes for the otogelin protein. We estimate about 15% of familial Ménière's is caused by mutations in the OTOG gene.”
He believes gene therapy may be an option for these patients.
Pre-clinical models with human Ménière's genes
Prof Lopez-Escamez performed this research in Spain over a decade before the University of Sydney received funding in 2023 for a Ménière's laboratory and began a global search for the right person to lead it. As a leader in the genetics of Ménière's and tinnitus, he was the ideal candidate. He recruited a team of seven, planned to grow to 12 by 2025, which is producing the first transgenic humanised model of Ménière's to contain the same disease mutations shared by multiple unrelated families in Spain.

Prof Lopez-Escamez says: "The University of Sydney and the Kolling Institue have built an ecosystem for medical research that offers great opportunities to conduct translational research, particularly in the neuroscience area where amazing projects in neurodevelopment, neurodegeneration and pain are being developed. They have a genuine engagement with patient-oriented research and this facilitates the attraction of international students and researchers. This multidisciplinary and multicultural research environment is very unique in Sydney and I am very proud to be part of it.
“We will study the pre-clinical model to observe if they develop hearing loss, and will study their vestibular system, gait, and if they develop imbalance. This is a new hypothesis that hearing loss genes, but different mutations, may drive Ménière's disease.
“We know these genes are expressed in the organ of Corti. They encode for proteins essential to attach hair cell stereocilia to the tectorial membrane. The OTOG gene is in coding for a protein that is linking the hair cell to the tectorial membrane. The hypothesis is that we have a protein which can’t link between the hair cell and the tectorial membrane. We are going to test this hypothesis in the pre-clinical model.”
Another part of the hypothesis is that structural damage in proteins that link the stereocilia could make these patients sensitive to sound which may
Images: The Kolling Institute.
Section of the temporal bone (A) containing the organ of Corti (B), with a zoom (C) to identify the attachment of the hair stereocilia to the tectorial membrane. In the tip of the stereocilia, the red dots are the mechanotransduction channel that permit the entry of potassium ion and depolarises the hair cells.
Prof Jose Antonio Lopez-Escamez in the Ménière-Neuroscience Laboratory at the Kolling Institute.
trigger imbalance when they perceive a noise.
The team will investigate the effect of noise on hearing loss and imbalance in preclinical models.
Reference database
Another project is to build a website reference database that contains genomic information from patients’ blood tests which could enable genetic diagnosis in the future. The database aims to help researchers, doctors and ultimately patients.
“The anonymised database of human Ménière's disease data would include genomic, epigenomic , and transcriptomic data,” Prof Lopez-Escamez explains. “It will be like a reference portal to train researchers and a tool for doctors.
“Genetic testing is a very important step to get more knowledge about the basis of many diseases. My idea is that any doctor can upload a file on the website and compare individual patients’ data with the anonymised reference data that we have generated. It will be useful and accessible."
He is trying to negotiate agreements with other researchers around the world especially South Korea, Europe and the US because of the importance of having data from different ethnicities. Comparing genetic and epigenetic variations in Ménière's across different countries will facilitate the genetic diagnosis.
If his team can demonstrate the pre-clinical model develops vestibular symptoms and hearing loss, the next step is to do gene therapy in the model. Ultimately, human patients on the register would have already been tested and would be first in line for gene therapy in people, he adds.
Patient blood samples are being collected at two hospitals – Royal North Shore Hospital and Royal Prince Alfred Hospital – and the plan is to extend to other centres in Australia and worldwide. Three main genes have been identified, but there are many more to be discovered, he says.
Allergy, inflammation and migraine
Other causes of Ménière's could be an immune response disorder, he adds. The team has performed blood testing and observed that proteins called cytokines are elevated in the blood of some patients. It found interleukin one beta, which is related to chronic inflammation, was persistently elevated to abnormal levels. These patients have chronic inflammation and the immune response is over-activated. Certain types of hearing loss are also related to this immune response. There are several drugs that could be potentially used in autoinflammatory MD, but clinical trials have not been performed. Allergy is another type of immunological alteration they found is related.
“We estimate that about 30% of patients with Ménière's have high levels of IgE, immunoglobulin, related to allergy.
"This data from Spain and China, and independent studies, have identified a Th2 type (immune) response with elevated cytokines. Ménière's is different in different countries. It is not the same in Europe as in Asia. For example, South Korean data shows their Ménière's is related more to allergies than Europe’s.”
This could be an environmental factor that can be modified, he adds.
“For some patients, allergy can be very important, and regulation of allergy could be important for their Ménière's. For others, the immune response could be important,” he says.
“There is also an association of Ménière's disease with other autoimmune disorders such as rheumatoid arthritis, autoimmune thyroid disease and even psoriasis.”
Lastly, migraine is common in Ménière's patients and symptoms will be worse if migraine is untreated.
“The first thing you must do if a patient has migraine and Ménière's is to ensure they are properly medicated and treated for migraine. Control the migraine which also affects the vestibular system and makes a person more sensitive to motion and travel, and ensure patients have good sleep as this relates to levels of cortisol,” he says.
“Doctors must keep in mind we are treating patients, and this disease has several associated conditions, it is not the same disease for all individuals. We must consider that each individual has a different genetic and immune background, and different associated diseases. We don't have a magic pill that is going to work for everybody with Ménière's. For some patients some medication will work, one drug will be better. But for others there will be another way.”
Prof Lopez-Escamez says this is why it is important for patients and healthcare professionals to know which subgroup of Ménière's disease a patient has.
“If you have migraine disease, you must be diagnosed and treated, but if you are under the autoimmune category, or you have the disease diagnosed in early years, there is a high chance you have a genetic condition,” he says.
“The first five years are the most critical in terms of managing the patient. I do not recommend surgery in the first five years. I know that a lot of surgery was done in past years but now we are moving into more precision medicine using more specific drugs. Gene therapy is not far away and will be available for the next generation of patients.” The Kolling Institute is recruiting Ménière's patients for genetic testing at the institute. Any volunteer willing to participate can email [email protected].
The talented team working in the new Ménière-Neuroscience Laboratory at the Kolling Institute.
Impacts of OTC hearing aids
In October 2022 the US Food and Drug Administration created an over-the-counter category for hearing aids, allowing them to be sold from stores or online without prescription or seeing an audiologist. What impact has this had there and how may this influence Australia?

While Australia’s Therapeutic Goods Administration (TGA) says it has no current plans to change how hearing devices are regulated in Australia, it says that over-the-counter (OTC) hearing aids can be supplied here subject to its approval. Several companies are already doing so.
In America, the FDA says it created the category to overcome barriers such as high cost, stigma of being perceived as old or debilitated, and value (perceived hearing benefit relative to price) as well as to increase access to hearing assistance allowing consumers an additional option for addressing their hearing health. Its justification was that nearly 30 million adults living in the US have hearing loss but only about one-fifth who could benefit seek a hearing aid intervention.
The FDA classified OTC hearing aids as medical devices and electronic devices for people aged 18 and over with perceived mild to moderate hearing loss. Buyers do not need a prescription, fitting by an audiologist or a medical examination and sellers do not need to be licensed. The devices may be bought in-person, by mail or online without involvement of a licensed hearing healthcare professional.
There are two categories; those with basic features such as volume control and a few predetermined settings; and self-fitting versions which allow consumers to customise their fitting and program device settings to suit their hearing needs through technology including software. This category must be reviewed by the FDA before sale via premarket notification. People do not need to provide age verification or measurements of
hearing loss to buy OTC hearing aids.
“We intend to provide reasonable assurance of safety and effectiveness for these devices as well as foster access to, and innovation in, hearing aid technology, thereby protecting and promoting the public health,” the FDA says in a statement on its website.
The FDA regulations require certain information on the outside of the box for OTC hearing aids. These include warnings against using them if under 18, advice on when to seek health care services, red flag conditions, and symptoms suggesting perceived mild to moderate hearing loss.
Overall positive move
Leading American audiologist Dr Steve Taddei says the move has had good and bad effects. While it has increased overall hearing health awareness, it has also confused consumers. His company found the audio performance of OTCs varies and while some can offer similar benefits to prescription hearing aids for mild-to-moderate hearing loss, others can potentially worsen speech clarity. But overall, he says it is a step in the right direction with many positive changes to consumers and the field.
Dr Taddei is co-founder and lab director of HearAdvisor (HearAdvisor. com), an independent test laboratory, where he works as an audiologist. He is also an audio engineer and teaches audio production and hearing sciences at several universities.
“Our team of two audiologists and one hearing scientist came together based on barriers we observed with the roll-out of over-the-counter hearing
Many over-the-counter hearing aids have been tested in the independent HearAdvisor lab.
aids,” he told Hearing Practitioner Australia (HPA). “We have tested more than 70 prescription and over-the-counter hearing aids and advanced earbuds since we launched in 2022. Our goal is to offer consumers objective and unbiased information regarding hearing aid audio performance.
“Since the 2022 over-the-counter ruling, the hearing aid market has seen an influx of new companies and products, along with heightened media

coverage and increased overall hearing health awareness.
“While these developments have been beneficial, confusion has also grown as consumers struggle to understand this new category and determine which devices, if any, are suitable for their hearing needs.
“Many people face challenges finding unbiased guidance in their search for better hearing. Among these challenges are affiliate-driven websites and companies using similar marketing claims for their products, which can be particularly confusing given that prices range from under $100 to several thousand dollars per product.”
Dr Taddei says the HearingTracker.com industry map highlights how confusing the market has become based on the number of companies alone.
“One thing we are finding is that the audio performance of OTC products varies almost as much as their prices,” he told HPA. “ To date we have objectively tested more than 70 hearing products in our lab, and while some OTC hearing aids can offer similar benefits to traditional prescription devices for those with mild-to-moderate hearing loss, others can potentially worsen speech clarity.
“Not surprisingly, the worst performers tend to fall in the sub-$500 category," he adds. " Products priced between $500 and $1000 show a wide range of performance, whereas those above $1000 generally offer the best audio quality.”
Minimal impact on prescription sales
Dr Taddei says, looking at the industry as a whole, OTC sales appear minimal and have had little impact on the prescription market.
“According to the (American) Hearing Industries Association (HIA), OTC sales accounted for only 1% of the overall 9% increase in hearing aid sales in the first quarter of 2023 compared to the previous year,” he says.
This is equivalent to at least 13,000 OTC hearing aid sales from January to March 2023.
“The 2022 ruling was a step in the right direction and has brought many positive changes to both consumers and the field,” Dr Taddei adds.
“It is important to note that OTC hearing aids are still in their infancy, so while barriers exist, we expect to see long-term benefits in terms of quality technology and consumer hearing outcomes.
“In the meantime, we should strive for better consumer protection and higher quality standards across all hearing products.”
Meanwhile, the first market survey in the OTC space to determine the public perception is being planned for late 2024 in America, according to Ms Bridget Dobyan.
Dobyan is executive director of the Hearing Industries Association (HIA) and was speaking to American thought leader in hearables and hearing health, Mr Andrew Bellavia on This Week in Hearing podcast on 6 June 2024.
The HIA is a forum for hearing aid manufacturers, suppliers, distributors, and hearing health professionals in the US and the only association in the US to represent hearing aid technology.
Its members are responsible for most of the more than four million hearing aids that are bought in the US annually. Its MarkeTrak survey collects data on hearing loss and hearing aid usage.
“Our next MarkeTrak will be fielding later this year with results expected in 2025,” Dobyan told This Week in Hearing
“MarkeTrack 2025 will be the first survey in the OTC space and we’re looking forward to this potential to obtain additional insight into OTC and consumer behaviours and perceptions, and if they have shifted in the last couple of years in this new reality.”
Its 2022 survey sampled 15,000 households including 3,218 people with hearing difficulty.
HIA warns that online descriptions of OTC hearing devices may not include all information required to be on packaging and suggests searching for reviews of the manufacturing company to ensure others have had a positive experience with the device and customer service.
Audiologist Dr Steve Taddei testing in the HearAdvisor lab.

Australian situation
A Department of Health and Aged Care spokesman told HPA on 22 July 2024 that the TGA has no plans to change how hearing devices are regulated in Australia and that subject to its approval, hearing aids can already be supplied OTC.
“In Australia, hearing aids are considered medical devices and require TGA approval before being supplied - regardless of whether they are sold over the counter (OTC) or prescribed by a health practitioner,” the spokesman said. “Subject to the TGA’s approval, hearing aids can already be supplied OTC in Australia. The TGA has no plans to change how hearing devices are regulated in Australia.”
OTC hearing aids are being sold including by audiologists, audiology practices and online.
Australian audiologist Ms Suzanne Porter and audiometrist Mr Don Hudson founded PocketAid, a direct-to-consumer hearing aid provider in 2024 after they saw a gap in the market for a “broad prescription and ready-to-use hearing aid”. They originally developed the hearing aid for audiologists to lend patients awaiting their prescription devices but said many customers reported that these outperformed the prescription hearing aids that had cost them thousands of dollars.
Porter and Hudson used hearing test results of more than 1,000 people with hearing loss to design PocketAid backed by research. “Our hearing aids are powered bys technology which we developed in-house; a broadly prescribable and automatic way of enhancing sounds, catering to everyday needs of the majority of those with hearing loss,” Hudson says.
“We’re aiming to improve accessibility for the vast majority of people who suffer from hearing loss and reduce the stigma associated with hearing aids. The products we’ve designed mean Australians can address their hearing needs and difficulties quickly with ready-to-use hearing aids straight from the box without the need for in-clinic appointments, and at significantly less cost.
"By simplifying the process and providing accessible solutions, PocketAid aims to increase hearing aid adoption and diminish stigma associated with hearing aids.”
Earlier, in March 2023 WS Audiology launched Vibe self-fitting OTC hearing aids in Australia online and at selected hearing clinics in major cities. They are registered medical devices, connected to a smartphone and controlled with a smartphone app. Within five minutes they can be
personalised to a user’s preference and hearing needs, the company
South Australian clinic My Hearing sells Vibe, marketed as a “cheaper, self-fitting hearing aid” manufactured using German technology. My Hearing says: “They suit anyone looking for a more affordable option or individuals who aren’t quite ready to commit to a prescription hearing aid.”
Summerlin Audiology in Perth sells OTC hearing aids but only recommends them after a hearing assessment, saying they have had mixed reviews in America and were originally designed to be a cheaper alternative to traditional hearing aids for ‘first-time’ users with mild hearing issues.
“They have to comply with many safety aspects regarding over-amplification running the risk of further damaging hearing and their fitting may mask ore sinister problem with hearing that could require surgery,” its website states. “Locally, a few models are available in Australia. Most will connect to a smartphone via a dedicated app to allow a quasi-hearing test to be undertaken with the earpieces in the ears. The smartphone then becomes a remote-control device for the OTC aids.
“The lower OTC hearing aid cost does not include any other services or appointments and so creates a dilemma for hearing care practitioners. We do have OTC hearing aids available but would only recommend these after a hearing assessment (to make sure there are no medical contra-indications) and discussion about lifestyle needs. We don’t want to risk a poor fitting and total rejection of hearing aids for the next seven years.”
Audiologist Iain Summerlin told HPA: “Although there have been quite a few views of the OTC entry on our website, there have been very few direct enquiries for these products. We do have patients with hearing levels within the normal range but difficulties hearing in background noise; OTC aids may offer an easy solution when occasional amplification is required. This strategy may also apply to first time users with a mild hearing loss. We have the Vibe from WSA; the ConC 400 from Sennheiser and the iQ buds to offer/ discuss as an option to traditional hearing aids for those hesitant to jump into amplification due to commitment issues or costs.”
OTC hearing aids ‘for mild to moderate heating loss or tinnitus’ are available without a script from Hearing Aid Australia shop, Ear & Hearing Australia independent Melbourne audiologists, and manufacturers are selling OTC hearing aids to consumers via brand websites or third-party retailers.
Studies on OTC devices
Two recent studies suggest there’s no difference in overall hearing aid outcomes between users of prescription and OTC hearing aids for mild to moderate hearing loss. However, some authors from both of the studies disclosed relationships with the HearX group, owner of Lexie Hearing which offers OTC hearing aids, and HearX helped fund one study.
The comparative effectiveness research study, published in July 2024 in JAMA Otolaryngology Head & Neck Surgery, “demonstrated self-fit over-thecounter hearing aids can offer comparable long-term benefits to audiologist -fit hearing aids for individuals with mild to moderate hearing loss”.
The study of 44 participants found no significant differences between

“We have objectively tested more than 70 hearing products and while some over-the-counter hearing aids can offer similar benefits to traditional prescription devices for those with mild-to-moderate hearing loss, others can potentially worsen speech clarity.”
Dr Steve Taddei HearAdvisor
Image: Steve Taddei.
Image: Peakstock/Shutterstock.
Over-the-counter hearing aids are marketed in America for those with mild to moderate hearing loss.

self-reported benefit of a self-fit OTC hearing aid and audiologist-fit hearing aid eight months after fitting.
“OTC may be an effective long-term intervention option for people with mild to moderate hearing loss. These results contribute to the growing body of literature supporting the feasibility and effectiveness of OTC hearing aids,” the researchers wrote.
The previous survey in 2022 of 406 prescription hearing aid users and 250 who used OTC models was published in The American Journal of Audiology It also concluded there was, “no significant difference for overall hearing aid outcomes” between clinic-prescribed and fitted hearing aids and OTC devices. But for the “daily use” domain, prescription clients reported significantly longer hours of daily use and for the “residual activity limitations” domain, OTC users reported significantly less difficulty hearing in situations where they most wanted to hear better.

However, Dr. Taddei cautions that these studies only examined one OTC product. Since performance and features vary among different devices, he says the results should not be generalised to all OTC hearing aids.
Audiology Australia view
When the FDA ruling came in 2022, Audiology Australia (AudA) issued a document on its consumer hub at audiology.asn.au/consumer-hub. This said it supported provision of hearing devices for all people diagnosed, through appropriate clinical consultation, as benefiting from the assistance of a hearing device.
It acknowledged some people may be interested in self-fitting hearing devices as a solution to managing their hearing loss or perceived hearing difficulty and developed a guide to help them understand some of the challenges associated with purchasing, fitting and adjusting a self-fitting hearing device.
“In all cases, AudA recommends the involvement of an accredited audiologist in the diagnosis of hearing loss or a self-perceived hearing difficulty, and in the support of clients, either face-to-face or through teleaudiology, with the adjustment of their preferred hearing device,” it said.
“It is important to note that hearing aids imported by individuals for personal use may not necessarily be regulated by the TGA. In Australia, the TGA regulates the sale of hearing aids for safety, quality and performance. In light of the new regulatory class of OTC hearing aids in the US, it is likely the TGA will review its current hearing aid regulations to decide if a similar regulatory approach will be taken in the supply of self-fitting hearing aids in
Australia" the AudA consumer statment said.
“If the TGA decides to approve for the regulation of a separate category of hearing aids that can be purchased over-the-counter without the involvement of a hearing health professional, the OTC hearing aids will be subject to TGA regulatory requirements for safety, quality and performance, and listed on the ARTG as medical devices.”
This listing would help individuals ascertain which OTC hearing devices were specifically designed for hearing loss and separate these products from personal sound amplifiers, which are not regulated by the TGA and generally not intended for hearing loss.
“If the TGA does not decide to approve for the regulation of OTC hearing aids, individuals in Australia will still be able to purchase and/or import the OTC hearing aids developed for the US market for personal use, either online or through a local supplier,” Auda said.
“AudA understands that self-fitting hearing devices may assist some clients with the self-management of milder hearing loss or with the amplification of sounds in certain situations. The use of self-fitting hearing devices may also represent convenience, autonomy and a financial saving. "
However, AudA recommends that anyone seeking to purchase a self-fitting hearing device considers their requirements carefully and ensures that, where they may need support for the fitting and adjustment of their hearing device, they seek the involvement of a qualified hearing health practitioner.
To safeguard long term hearing health, AudA strongly recommends that an audiologist is involved in the assessment of hearing ability before the purchase of a hearing device, which include self-fitting hearing devices. AudA further encourages clients to take action to ensure that the products that they are purchasing are done so through a reputable supplier after they have sought appropriate advice and diagnosis from an accredited audiologist to ascertain that a hearing device is the best support for their individual circumstances.”
Some over-the-counter hearing aids, such as the PocketAid Jasper 3 Dura, are being sold in Australia. Image: PocketAid.
Image: Monika Wisniewska/stock.adobe.com.
Changing lives one ear at a time
SIMONE CHEADLE has helped change the lives of hundreds of Australian families and their children who were born with microtia and/or atresia. Fate put her on this path after her daughter Chelsea was born with the conditions.
Every year roughly 30 babies (one in 10,000) are born in Australia with microtia - an incomplete or underdeveloped ear - and/or atresia - a missing or closed ear canal, with resulting hearing problems. In most cases they occur together.

When Brisbane mum and former teacher Mrs Simone Cheadle’s third child, Chelsea was born 20 years ago with both conditions, there was barely any information or support, and limited treatment options for these children.
But over the past two decades Simone's resilience and persistence has put Chelsea on the best path to reaching her potential and a fulfilling life. Simone has since dedicated her life to helping others and changing the trajectory of their journey towards positive outcomes.
Babies are identified at birth and are now offered referral and treatment, she says. The 90% with unilateral hearing loss are offered fully subsidised bone conduction devices through Hearing Australia. Patients also have choices for ear reconstruction with both reconstructive techniques available in Australia;’ a traditional rib graft method or newer technology using 3D customised ear implants to create a 3-dimensional ear that mirrors their other ear.
It’s a far cry from the support and services that were available 20 years ago when Simone had to argue, persist and go overseas in 2008 for surgery for Chelsea as no practitioners in Australia offered the solutions she had found.
Simone has helped change that, bringing options, information, hope, support and resources to families struggling with the diagnosis and not knowing what is ahead. Connecting families and providing opportunities for children with microtia and atresia and their parents to meet and support each other helps them feel less alone in their journeys, she says. Early intervention services can also assist in monitoring their child’s developmental milestones and optimising their outcomes.
“When Chels was born we weren’t even told the name of the conditions. Her paediatrician was flipping through a book and came up with ‘malformed ears.’ It wasn’t until we went to the ENT surgeon when she was five months old that we were given the names,” she recalls.
“There was no Facebook or Google so it was difficult to get information. I didn’t know these conditions existed before she was born. I did a yahoo search for ear malformations and it gave a list of linked conditions such as

cognitive delays, spinal issues as well as heart problems, so not having correct information was stressful.”
‘Cried every day since he was born’
Finding other families was hard without today’s online connection but she found families in Melbourne, Sydney and Adelaide via an MSN group and they connected via email and phonecalls.“The mum of a baby boy called and we spoke for two hours. She later said, ‘I cried every day since he was born until I spoke to you and then I haven’t cried since.’ It gave me this feeling that I'd really helped and it was such a good feeling, there was nothing like it. She’s now one of my best friends.
“The people we met and amazing connections we made was the start of our support network. I’d done lots of research to educate myself, talked to many parents and followed international families’ blogs documenting their surgical journeys so I could understand microtia and atresia and we could come up with the best course of action for Chelsea and I thought it’s silly for me to not share that information.
“We’ve done a lot to raise awareness and information so hopefully that path’s easier now.”
When Chelsea was a baby, her Mum took her to see founder of Hear and Say, Dr Dimity Dornan, a speech, listening and spoken language specialist who specialised in hearing loss. “Talking to her put my mind at rest and gave me hope that everything was going to be okay. She was the first professional who explained impacts of hearing loss and gave practical information," she says..
“Through her I met two Queensland families. I wrote letters and being the persistent mum I was, I urged us to start a support group. At our first meeting everyone just cried because it was a relief to find others.” Simone had contact with parents in an international group and began hearing about surgeons overseas who were getting good results. She made inquiries in Australia but was met with closed doors.
“The Australian surgeons only offered the rib graft ear reconstruction and the surgeon we saw was not confident of a good aesthetic result, which was disheartening,” she recalls. “I asked about opening the ear canal because it was being done overseas but the advice was they didn’t do it here and as she had hearing in one ear, that was enough. “I had read that unilateral hearing loss had a significant impact so I couldn't sit there and do nothing. I’d seen there were new devices being trialled in Europe and I was deflated because no-one could say when they would come here.” Chelsea was offered a Bernafon bone conduction aid on a metal headband. Her Mum adapted soft headbands to incorporate the hearing aid and make it comfortable.
Porous implant so blood vessels grow through
At age four, Chelsea attended California Ear Institute for atresia repair surgery followed six months later by a newer procedure for ear reconstruction using a synthetic polyethylene implant.
Images: Microtia Atresia Australia.
Baby Chelsea Cheadle.
Chelsea Cheadle and her mum Simone Cheadle have helped hundreds of children with microtia and atresia throughout Australia since Chelsea was born with the conditions.
“The polyethylene implant is inert, so it’s tolerated well, porous so blood vessels grow through and it has a blood supply. It had been used in other parts of the body for decades,” Simone recalls.
The implant was suitable for children from age four whereas the cartilage method required an older child with a big enough rib circumference to harvest sufficient cartilage to construct an ear, and was usually performed at eight to 12 years of age. Being an ex-teacher Simone didn’t want her daughter to be self-conscious at school or for it to affect her self-esteem.
“She had a bubbly, vibrant personality and I wanted her to stay true to that and not get to a point where she’d be concerned about her ear so we did it before school,” she says. “That's a motivating factor in surgery for many families so the child can start school looking like their peers.”
The dedicated mother quit teaching to work for Hear and Say establishing and co-ordinating a microtia atresia support program. From 2009 she organised annual conferences - the American surgeons spoke at the first oneand she continued for 13 years until the program ceased. In 2022 she founded Microtia Atresia Australia.
“I’m passionate about continuing to help children with microtia and atresia and their families because these families continue to need up to date information and support, and there is nowhere else they are able to get this,” she explains.
The organisation provides a website with information for parents and health professionals about microtia, atresia, hearing loss, speech and language, NDIS and treatment options. It offers an online learning library with on-demand presentations, family support and planning meetings, webinars, fact sheets and an online support group. It facilitates confidence and resilience workshops for school-aged children with microtia and atresia and provides resources including children’s books and bone conduction headphones.
“We continue to host several conferences a year in different states and have an online conference,” Simone says. “This is my 16th year organising them and we’ve had hundreds of families attend.
“They provide a unique opportunity for parents and professionals to hear about the latest information relating to microtia and atresia from some of the most experienced professionals nationally and internationally. We have presentations on audiology topics, speech and language, social and emotional impacts, parent support including advocacy, ear reconstruction, and updates from companies who manufacture devices for these children such as Cochlear, Oticon Medical and MED-EL. We always hear from parents and children or adults born with microtia and atresia.”
Psychologist Evelyn Field OAM, author of the book Bully Blocking, is a speaker at this years’ conferences, discussing effects of bullying and providing strategies to combat it.
When children receive their hearing aids from Hearing Australia, much time is taken with testing, interpreting and adjusting devices so there's not a lot of time to talk to families about specific features, Simone says. At the conferences hearing aid manufacturers discuss settings, features and accessories, giving a better understanding of devices and how to maximise potential. A family fun day/picnic follows to enable families and children to meet and mix socially.


a child with microtia and atresia. Parents buy them to read to their children and send them to school or kindergarten for teachers to read to their class.
Feedback indicates how valuable the conferences are. "We receive positive messages from families saying things like, ‘with all the specialists we see, no-one's ever given us this information,’ and another Mum sent a message saying she’d talked to her child's kindy teacher about what she'd learnt at the conference and how they could help her daughter.”
While the decision for surgery is big, it’s a small part of the journey. “It’s the day-to-day stuff, dealing with hearing loss, its impacts including in the classroom, their self-esteem, building resilience and confidence so my focus at conferences this year is supporting school-age children,” she says.

“The conferences provide information to help parents make informed choices for their children but the picnic is so families can connect socially and parents can meet and have that parent-to-parent support which is so important. It’s a rare opportunity for the children to meet too,” Simone adds. “They can see other kids with little ears, reconstructed ears, wearing bone conduction devices and you hear comments like, ‘Mum that boy has a hearing aid like mine’ or ‘that girl has an ear just like mine.”
Children’s books with characters like them
Through the Facebook support group, parents said there were no children’s books kids could relate to featuring characters with their conditions so Simone wrote and published two. One is about how Chelsea explains her ear to her friends and the other about her undergoing surgery. Chelsea and her sister illustrated one when they were young, and the other is illustrated by a mother of
Parents can use NDIS funds to pay for conference attendance and consultations with Simone to advise about what else the funds can be used for including assessments, interventions, therapy, audiology, hearing loss strategies, individual goals and training to build independence, resilience and self-confidence. She has provided professional development to audiologists and hearing screeners and receives calls advising when a baby is born with microtia/atresia asking if staff can give the family her details.
Simone's motivation for providing support and services to families is simple. “I want them to have all the information and support that I didn’t have when my daughter was born,” she says. “I still talk to families who are struggling emotionally and unfortunately there are lots of children with microtia and atresia who are doing it tough emotionally and struggling with self-esteem, confidence and resilience. There are things I can do to make theirs and their parents’ journeys a little easier.” She is committed to making a difference for these children and passionate about helping families optimise outcomes by providing information, services, support, resources and advocacy.
Following in her Mum’s helper footsteps, Chelsea is studying occupational therapy and working part-time in a hospital OT department, due to the desire to help and inspire others as she has been helped on her incredible journey.
These Australian boys wear bone conduction devices to assist their hearing. They and their families have received support from Microtia Atresia Australia.
Families at a Microtia Atresia Australia gathering.
Innovative 3D printed ears
Reconstructive plastic surgeon DR JOE DUSSELDORP from Sydney performed the first custom 3D ear implant in Australia in 2019 on four-year-old Brisbane boy, Maxim Richter, who was born with microtia and atresia.
A year later he performed the same surgery on another boy, Sebastian Orellana, who became the first to receive the 3D ear implant combined with a Cochlear BAHA-Attract implant (bone-anchored hearing aid) for his atresia. Sebastian’s father, Carlos, says Sebastian went from being withdrawn and sometimes bullied at school to a child who was no longer self-conscious of his facial difference, and who has since taken on leadership positions in his school.
Sebastian has spoken openly about his journey on social media and television and recently underwent a revisionary surgical procedure to upgrade his hearing implant to the Cochlear OSIA device, a different form of active implantable bone conduction hearing aid.
Since then, Dr Dusseldorp has performed the surgery on another 16 children, aged between four and 12, and two adults from around Australia with microtia and atresia. About half of these patients chose to have the BAHA implanted at the same time.
Maxim also had hemi-facial microsomia, where one side of the face is smaller than the other side. This condition can be associated with microtia and atresia.

Dr Dusseldorp says: “I performed a reconstruction of his ear using an implant made from a biocompatible polymer material, known as Su-Por, a type of porous polyethylene made by US-based company Poriferous and distributed in Australia by Lyka-Smith. The implant was modelled from a mirror image of Maxim's other normal ear. We also used 3D imaging to plan the ideal positioning of his new ear, which can be challenging in cases of facial asymmetry.
“It will reassure other families like Maxim’s that these advances in microtia surgery, which aim to improve outcomes for their children, can be performed here in Australia.”
10-hour surgery
The custom 3D printed technique has several advantages over the previous rib grafting technique; it can be performed with less pain and time in hospital, and at a younger age often before starting school.
Dr Dusseldorp uses the patient’s healthy ear as the model so the implanted ear can be made identical in shape and size. He does this by using an optical surface scanner to render the 3D shape of the healthy ear and then digitally creating a mirror image 3D file which can be used to create a 3D printed mould. The porous polyethylene material is then injected into the 3D printed mould to create a mirror-image replica of the healthy ear. The custom 3D ear implant is then surgically implanted in a technically-demanding surgery that can take eight to 10 hours.
Microtia Atresia Australia founder Ms Simone Cheadle recalls: “One of Dr Dusseldorp's patients had a uniquely shaped ear and he asked the boy’s parents if they wanted him to adjust the shape of the new ear but they said no, that was his ear and they wanted it matched exactly.”
Dr Dusseldorp adds: “The innovation landscape is full of opportunity to


combine technological advancements with modern clinical practice. Translating these advances to clinical application is the most rewarding part of my work because this is when you see how research changes lives.
"As a father myself, I know the powerful emotions a parent experiences when their children require medical attention and being able to offer improved solutions and better outcomes to wonderful kids like Maxim and Sebastian and their parents is very fulfilling.”
In 2020 when Maxim started school his mum, Maria, said: “We wanted Max to go into school looking like all the other kids. I feel that the ear reconstruction played a paramount part in Maxim’s confidence and helped him achieve a sense of belonging with his peers.”
Dr Dusseldorp studied under some of the most talented surgeons in the world and has honed his skills as a reconstructive plastic surgeon from Vietnam to France and most recently in the USA.
Simone adds: “Dr Dusseldorp is one of the most qualified and experienced surgeons in this field in Australia and has been mentored by the American pioneers as well. He is specialised in using the same polyethylene material as Chelsea’s ear however her implant was in two pieces with the outer rim and inner rim framework joined together. The implants today are in one piece and are stronger.
"Chels’ ear reconstruction was 15 years ago and is older technology but the implant has stood the test of time. We are still happy with the results and no-one would know she’s had a reconstruction.
Dr Dusseldorp regularly speaks at Microtia Atresia Australia conferences and has recently presented in Melbourne to outline some of the potential risks of this new procedure. Given that the material is biocompatible but not truly biological, there can be risks of foreign body reaction and the risk of need for revisionary surgery at some point in the life of the implant is quite high.

A close collaborator with Dr Dusseldorp is Sydney ENT specialist, Associate Professor Payal Mukherjee from the Royal Prince Alfred Hospital. As well as being the ENT surgeon who has implanted almost all of the BAHA devices for Dr Dusseldorp’s patients, Associate Professor Mukherjee is part of a team researching and developing technology using a 3D bioprinter developed at the University of Wollongong. This reconstructs ears made from patients’ own stem cells so there is less chance of rejection.
She is also developing a 3D printed living ear using living cells. Studies are underway to see if the bioprinted cartilage could give the same strength and hold the same shape as current treatments and once ready clinical trials will be on the horizon.
“There is always room for us to look at making these procedures safer and more reliable and the promise of 3D bioprinting cartilage is very alluring and something we would all love to see become a viable treatment option for children like Maxim and Sebastian,” Dr Dusseldorp says.
ABOVE, L TO R: Surgeon Dr Joe Dusseldorp with happy patient, Sebastian Orellana; Sebastian
ABOVE, L TO R: A 3D printed earmould for Max’s surgery; Dr Dusseldorp performing the technically demanding eight- to 10-hour 3D ear implant surgery.
Images: Dr Joe Dusseldorp.
50 years of outstanding education for audiologists

The University of Melbourne has celebrated the 50th anniversary of the launch of its audiology degree, the largest and oldest course of its kind in Australia. Many have passed through the hallowed halls of the esteemed institution and graduated as audiologists.
The University of Melbourne audiology course was pivotal in laying the foundations for the audiology profession in Australia and further developing it. From just 12 students in the inaugural 1974 cohort, it has grown significantly to match demand with 82 first year students in 2024. In the past five decades, it has sent thousands of audiologists into the world to improve the hearing health of the nation.
It was the first university to offer an audiology course in Australia and New Zealand. After Professor Graeme Clark’s appointment as the Professor of Otolaryngology at the university in 1970, he led the creation of the course which launched in 1974 as a one-year graduate diploma.
Head of the Audiology and Speech Pathology Department Associate Professor Dani Tomlin says the course was introduced due to an increasing need for people who understood the science of hearing and how it was relevant for patients clinically.
The university decided to offer graduate training in audiology to reflect this work as a more clinical profession, joining the existing Department of Otolaryngology in the faculty of Medicine, she explains. It changed to a two-year Master of Clinical Audiology program in 1998, with the first students graduating in 1999.
“We are proud of the role that the course has had in further developing the profession, including its role in early cochlear implantation research and laying the foundations for the profession in Australia,” A/Prof Tomlin tells Hearing Practitioner Australia
Mr Field Rickards, (later Professor Rickards) was appointed its first lecturer in 1973 to teach the 1974 cohort and remained a lecturer and then senior lecturer until 1989. Initially there were only a few lecturers, with just one to two for the first few years, compared to today’s staff of more than 20.
“When setting up the audiology course, there was an emphasis on
producing graduate audiologists with a strong understanding of integration of results and appropriate management of hearing conditions,” A/ Prof Tomlin says. “Changing technology has altered many audiologists’ roles. Advancements in areas such as hearing aid and cochlear implant technology and testing using evoked potential testing allows many different options for audiologists to be involved in while assessing and managing hearing healthcare.”
An audiology clinic was set up in 1975, as part of the Department of Otolaryngology, primarily seeing a small number of private patients. “The clinic has changed to run as a busy private clinic run by Melbourne Teaching Health Clinics, providing clinical placements to students and service to clients across many audiological aspects, including paediatric, adult rehabilitation and vestibular clinics,” A/Prof Tomlin says.
A bright future
Today’s curriculum includes more than just clinical skills, now incorporating current health themes, interprofessional practice and person-centred care to ensure graduates are well prepared for practising in a changing health environment.
“The Master of Clinical Audiology, a two-year entry to practice degree, prepares graduates for professional practice in the space of hearing and balance disorder detection and management,” A/Prof Tomlin says. Through the initiatives and innovations of the teaching team, themes of communication, professionalism, First Nations health, global audiology and
ABOVE: The inaugural, 12-strong 1976 graduation cohort (left), with staff including first lecturer Mr Field Rickards (centre front) and course instigator Professor Graeme Clark front far right; the 2023 graduate group (right). Images: University of Melbourne.
Images: University of Melbourne.

TIMELINE
1970: Prof Graeme Clark appointed Foundation Professor of Otolaryngology in the Faculty of Medicine; began establishing Australia’s first university audiology course.
1974: Initial student intake of 12; many working as audiologists with a psychology degree.
1978: Prof Clark performed the first Melbourne cochlear implant operation at The Royal Victorian Eye and Ear Hospital.
1990: To provide extra placement opportunities in all audiology areas, the university clinic expanded to include a private clinic (Academic Hearing Aids).
1994: Moved from 10-12 Morrison-Pl to 172 Victoria-Pde, East Melbourne.
1999: First graduating cohort from the Master of Clinical Audiology course.
2001: Richard Dowell appointed first Professor of Audiology and Speech Science in the Department of Otolaryngology.
2009: Moved to the current location, 550 Swanston-St Carlton co-located with The Hearing Cooperative Research Centre (HEARing CRC) until 2019.
2012: Speech pathology joined the department, and the Department of Audiology and Speech Pathology was established.
2013: The department joined the Melbourne School of Health Sciences.
2019: Professor Gary Rance appointed Head of Department of Audiology and Speech Pathology.
2022: Dani Tomlin appointed Head of Department of Audiology and Speech Pathology.
interprofessional practice have been woven into learning opportunities for students whilst clinical skills develop.
“It is through this program that the teaching team has ensured a course that fosters professional, compassionate, global citizens with a person-centric focus,” A/Prof Tomlin says.
The audiology teaching team has been recognised for different aspects of the course over recent years and in 2023, was awarded the university's Faculty of Medicine, Dentistry and Health Sciences award for sustained teaching excellence.
A/Prof Tomlin predicts education will adapt to reflect changes to the profession.“An increasing emphasis on person-centred-care and interdisciplinary practice has been introduced to the course to help better prepare students for the current profession,” she says. “The teaching team continues to excel in its approach to teaching and learning, whilst continually developing innovative approaches that align with the strategies of the university and values of the faculty.”
The team has established global partnerships with universities and health-care providers but has equally focused on the importance of local community partnerships with First Nations community-based health. These connections and shared teaching and clinical placement experiences ensure students leave the course with cultural experiences and a global perspective on health care, she says.
“The audiology team has a focus on interdisciplinary collaborative practice leading the way in multidisciplinary placement and teaching opportunities with physiotherapy, dentistry, optometry, social work, music, and speech pathology,” A/Prof Tomlin explains. “Final year students also undertake independent research study in collaboration with industry partners.”
In 2024, a new audiology curriculum was introduced for the first-year cohort to reflect changes in audiology practice, focussing on greater emphasis of professional practice. “While this new course aims to maintain excellent clinical skills, further emphasis is also placed on clinical communication,
Guests at the 50th celebration.

evidence-based practice, and First Nations healthcare,” A/Prof Tomlin says. While a Doctor of Audiology had been explored in recent years as occurs in America, it was felt that at the time “this was not appropriate for our local market; however, we are continually engaging with industry and alumni to ensure our course offerings are appropriate for the profession” she adds.

“The department is dedicated to shaping the future hearing health care workforce for the next 50 years.”
Celebrations a hit

More than 180 guests attended the 50th Anniversary of Audiology celebrations at Melbourne Connect in May 2024. The event kickstarted the first Inaugural Audiology Annual Conversation, which explored audiology’s role in increasing health span.
Dean of the Faculty of Medicine, Dentistry and Health Sciences, Professor Jane Gunn, and A/ Prof Dani Tomlin welcomed guests. Keynote speakers were Professor Julia Sarant and Professor Barbara Weinstein and a panel discussion including alumni and consumers of hearing healthcare was facilitated by Professor Bob Cowan. Invited speakers were Ms Sally Woods, Ms Jane MacDonald, Mr John Langford, Mr Matt Grounds, Professor Bruce Thompson, A/Professor Dani Tomlin, Professor Field Rickards, Professor Richard Dowel and Dr Sally Cockburn.
The discussion explored promotion of collaborative care, emphasising the importance of breaking down silos to deliver more holistic services in the healthcare system. Panellists also discussed artificial intelligence and necessary adaptations in audiology training, and networking occurred for alumni and professional peers to reconnect with former classmates and colleagues and engage with current audiology students.
A highlight was a video message from Professor Graeme Clark AC, Lasker Laureate.
“This anniversary is a 50-year milestone for the university’s audiology and speech pathology course and also a milestone for the discipline in Australia,” he said in the video swhich can be seen at healthsciences.unimelb.edu.au.
“Congratulations to you all. You have achieved much more than we could ever have imagined.”
In the 1960s, ENT surgeons performed audiometry in their back offices and CAL (the Commonwealth Acoustic Laboratories), later NAL (the National Acoustic Laboratories), had psychologists do speech tests for hearing aids. “When I arrived in Melbourne in January 1970 to take up the Chair in Otolaryngology, I was greeted by highly motivated people who wanted to see change and university courses established. Chief among those movers and
developing the profession, including its role in early cochlear implantation research and laying the foundations for the profession in Australia.”
A/Prof Dani Tomlin Department of Audiology and Speech Pathology
shakers was Mrs Nancy John (founder of the Advisory Council for Children with Impaired Hearing),” Prof Clark said.
“Our group moved into action and formed a committee that convinced the state government that university training in audiology would improve standards and help the people. To make sure, the government invited Professor Ian Taylor from Manchester University to check us out. Then we had to convince the university that audiology had academic merit and it was finally approved in 1973.”
Prof Clark said he had a vision that future audiologists should be knowledgeable in the basic sciences and so his post-graduate student with a major in physics Prof Rickards was appointed to lead the course. “He did an outstanding job,” Prof Clark said. “Our first year was tough as we were teaching some senior audiologists, then over the next few years the course gained momentum and became very popular as a career.”
Simultaneously the department was doing research to see if electrical stimulation of the brain could help people understand speech. “When we discovered a cochlear implant was possible, the next big thing was who should clinically manage the patient?” Prof Clark said in the video. Fortunately there were now experienced audiologists with various scientific backgrounds and he paid tribute to all involved but mentioned the first two, Ms Angela Marshall and Ms Lois Martin.
When Cochlear developed the cochlear implant, he said the university became the main test centre and in 1982 Prof Richard Dowell was the audiologist who managed the first patient to receive a commercial multi-channel cochlear implant, Mr Graham Carrick. “We became a united group studying diagnosis and treatment of hearing loss. In 1985 we implanted our first young child Scott Smith and again audiologists played an essential role. I congratulate all audiologists for selecting this career and may the course go from strength to strength."
Past alumni with an example of a previous generation of audiometer.
Prof Bruce Thompson, head of the university’s School of Health welcomingSciences, guests to the 50th celebrationanniversary event.
NEW 60/60 RULE ‘A REVELATION’ IN CI REFERRAL
DR BRENT MCMONAGLE explains how we can all make efforts to improve the number of adult cochlear implant recipients.

ONLY 11% OF ADULTS (ELIGIBLE FOR COCHLEAR IMPLANTS) ARE IMPLANTED WHICH IS VERY DISAPPOINTING AND TOTALLY UNACCEPTABLE. DR BRENT MCMONAGLE
Cochlear implants (CIs) are one of medicine’s most important technological advances and are considered the gold standard treatment for patients with severe to profound hearing loss when hearing aids aren’t adequate.
Despite this, significant barriers exist.
In Australia, about 90% of eligible babies are implanted but only 11% of adults are which is very disappointing and totally unacceptable.
CIs are available through the public system, Department of Veteran Affairs - for some white card and all gold card holders - and for most privately insured patients. Twelve years is the average time between when someone becomes eligible for a CI and they receive one which is 15% of the average lifespan!
Once aware they are eligible, 90% proceed to cochlear implant surgery within a year.
The reasons for this lack of penetration are complicated and multifactorial.
The major reason relates to referrals. CI referral can come from GPs, audiologists and audiometrists, from patients themselves or concerned/ frustrated family and friends.
GPs bear the brunt of general health care and must be across almost all aspects of medicine.
Hearing loss is a poorly taught and understood component of medical school teaching and ongoing GP professional education.
In my opinion, there is a tendency for GPs to refer patients for audiograms and then presume the audiologist will suggest a hearing aid if appropriate and may then consider the management of the hearing loss has been passed onto audiologists and audiometrists.
Understandably, audiologists and audiometrists are the main referrers, at least in my practice.
From talking to audiological colleagues, there is apparently not much instruction on CIs during audiological training, and as such, some audiologists and audiometrists may not be aware of referral guidelines.
The recently described 60/60 rule has been a revelation in simplifying referral guidelines.
The 60/60 referral guideline for identifying patients who should be referred for a cochlear implant candidacy evaluation (CICE) states patients should be referred if they demonstrate a best ear unaided monosyllabic word score less than or equal to 60% correct and if they demonstrate an unaided pure-tone average in their better ear that is greater than or equal to 60 dB HL.

A referral for a CI doesn’t mean the patient will receive a CI; it’s just the next step along the path to determine candidacy. There may be concerns about referring “too early”, before a candidate is audiologically indicated. This is rarely a problem as the worst that can happen is the patient is counselled by CI audiologists, ENT surgeons or both about CIs and told that they are not ready yet but may well become eligible in the future.
Audiologists and audiometrists may also “hang on” to patients rather than broadening the management team by offering referral for a CI assessment due to reservations about “losing” patients if they opt for a CI.
If a new audiological team becomes involved and takes over the implanted ear, the audiologist can continue to care for the non-implanted ear, if aided
on that side. Finally, patients and family members also may initiate referral due to sheer frustration with worsening communication difficulties.
Age is rarely an issue: cochlear implantation occurs in newborn babies from six months of age into the 90s; in fact, the oldest CI recipient was 103! We cannot be ageist and assume that someone is too old.
Humans are living longer with each generation and people want good quality of life hence the increasing numbers of cataract operations, joint replacements and other procedures in the elderly.
Cochlear implantation is not a rarely performed operation anymore like it was in the late 1970s and 1980s. It is also not only for the bilateral, profoundly deaf; CIs are indicated for moderately severe to profound hearing loss where hearing aids are insufficient.
The operation only takes about two hours with one night in hospital - sometimes day surgery - and minimal pain. Most patients report a straight-forward recovery with the worst issue usually being some imbalance or rarely vertigo which usually settles within days.
There is also the long-standing issue of the stigma of hearing aids; some people have reservations about wearing hearing aids due to aesthetic concerns. While spectacles can be trendy and a fashion statement, hearing aids seem to project advancing age and disability.
Moving forward, we can all make efforts to improve the number of adult cochlear implant recipients. GPs and audiologists could potentially have more exposure to CIs in their training and ongoing professional development. Governments could help to promote hearing loss awareness more and improve access for hearing testing. Perhaps hearing loss could even become more prominent in GP screening programs.
ABOUT THE AUTHOR: Dr Brent McMonagle is a paediatric and adult ENT surgeon from the Gold Coast who specialises in cochlear implantation.
BELOW: Dr Brent McMonagle. Images: Dr Brent McMonagle.
FLY IN SYNCH WITH YOUR CUSTOMER
CHEDY KALACH and VIRGILIA READETT give some valuable tips on providing the best customer service for your patients.


TAKE THE RICHARDSTEP.COM QUIZ TO DISCOVER YOUR 'BIRD' AND THE CUSTOMER TYPE YOU FEEL MOST AT EASE SERVING.
CHEDY KALACH & VIRGILIA READETT
an you recall the best customer service you ever received? Did you feel like they were ticking boxes? Or did they “get” you? It probably felt effortless, like their service and product were tailored for you. That is because it was.
Adapting to the person you are serving has been at the forefront of customer service training for decades. How should we tailor our approach? What methods suit which customer? It can be trial and error. You’ll hit the mark for somecreating loyal customers but for others, it can seem a mystery. What do they want?
We’re drawn to those we have similarities or common ground with; look at your friendship circle or co-workers you click with. This can be applied to customer service in audiology and ‘mirroring’ can be the feather in a successful salesperson’s cap.
To mirror your customer and quickly and accurately profile their behavioural type, the first step is knowing how to respond to their category or “bird”. The D.O.P.E model – Dove, Owl, Peacock, Eagle - was developed by Richard Stephenson, based on the work of Dr Gary Couture and Dr William Marston.
Doves are natural diplomats; patient, sensitive, supportive and loyal, seeking a sense of belonging and wanting to feel like a supportive and caring member of groups. Logical, analytical and reserved are traits we associate with the owl. Owls look for predictability, they put logic before feelings and seek structure, facts and figures.
BELOW: Are you a dove, an owl, a peacock or an eagle?

The peacock – charismatic, outgoing and animated - prioritises people before tasks, seeking recognition and popularity.
Eagles are confident, ambitious, decisive and impatient, seeking results and looking for a challenge. Power and authority are high on their agenda. These traits have tell-tale signs in the audiological environment. The customer who sneaks in unnoticed and waits quietly until no-one else is waiting to ask for help; classic traits of the dove.
Owls are prepared with quotes and pamphlets, a list of devices they’ve researched and a question for every aspect of the dispense.
The clinic knows when a peacock arrives. They involve family, friends, every staff member and other customers in their selection and concentrate on the process rather than result. They may not have booked an appointment but will expect to be seen that day and are the perfect walk-in as they make fast, decisive selections and usually a same day purchase.
ONCE YOU IDENTIFY THE TYPE, HOW DO YOU ADAPT TO THEM?
Doves are high-risk as they talk with their feet and may never come back if they have adaptation issues, don’t like their hearing aids or don’t feel welcome. Let them make decisions but be pre-emptive about what to expect adapting to the device. Open the door for them to feel safe and welcome. If you win them over, they will be a customer for life.
Owls may seem time-consuming because they are. Pull out your arsenal to impress; detailed quotes and information, multiple methods to explain features and benefits, samples, digital displays or technical explanations. Jargon, if used correctly, will impress. If troubleshooting,


let them see the step-by-step procedure you go through, keep a checklist or fill in an adaptation or troubleshooting report. Impress them with technical explanations and they’ll continue to come back. Engage and assist peacocks. They want your guiding support but will confer with others; don’t feel offended if they don’t take your advice. They need to hear five other people tell them the same thing. Offer samples, make the experience hands on, pass options to try on. They thrive on interaction and enjoy having you talk them through the process. A happy peacock will be your biggest advocate. Eagles want concise explanation. Let them witness your efficient systems. Eagles value when you go the extra mile to find suitable appointments and inform them on timeframes. If you win them over, they’ll trust you to offer them the best device and options.
The common thread is people over product; even for decisive results-driven eagles, it is people who draw them back. Take the richardstep.com quiz to discover your “bird” and the customer type you feel most at ease serving. Your second highest score is the type you can easily access but your lowest two may take more effort to adapt to. Work as a team to let staff shine where they have the best potential to do so.

ABOUT THE AUTHORS: Chedy Kalach is director of the Australasian College of Audiometry. Virgilia Readett is a senior trainer with the Australasian College of Optical Dispensing.
College of Optical Dispensing.
Chedy Kalach
Virgilia Readett
MAKE MEETINGS GREAT AGAIN
KAREN CROUCH’S firm was once asked to sit in on a practice’s meetings and offer guidance on how staff can extract more from these interactions. Here’s what she found.

A DECISION THAT COULD BE MADE EASILY BY CIRCULATED EMAIL MIGHT ONLY REQUIRE A MEETING IF PARTIES INVOLVED CANNOT REACH AGREEMENT.
KAREN CROUCH
While meetings are often loathed for being time-consuming and unproductive, executing them well is pivotal for collaboration and organisational success. And there are many techniques to ensure meetings – not just one-on-one meetings but formal office forums – bring value to the practice.
Effective communication is essential to developing a well-coordinated, teamfocused environment. Conducting effective meetings – whether for educational or practice management purposes or general team building – is a key to maximise the effective communication effort.
Practices sometimes pride themselves on strong interpersonal communication based on the number of meetings. But on closer inspection, it’s clear they often lack the more important factors of quality and results.
Our firm was once requested to assess the effectiveness of a particular practice’s meetings to enrich the quality and ‘achievement value’ of these gatherings, improving decision-making, and promulgating meeting resolutions including enactment of the decisions.
Practice meetings were conducted between various job families: administration, clinicians and principals. Most felt the level of communication within the practice was high. However, most interviewees agreed that decisions were not always clear, or communicated effectively despite ample debate about issues in point.
This resulted in poor implementation of meeting resolutions.
With staff cooperation and input, we defined

the following attributes of an effective meeting:
• Ensure a planned ‘agenda’ to impart a clear understanding of subject matter and target outcomes
• Improve communication and decision making
• Exchange experiences, information and knowledge between participants
• ‘Work smarter’ (research) forums
• Implement decisions effectively including post-implementation reviews to assess success
• Complement and potentially improve corporate governance.
Some meetings for social purposes –such as Christmas party planning – were conducted on an informal basis, mainly for office planning purposes and for business/ relationship development efforts. Generally, content was less structured, albeit well planned beforehand. Such gatherings were obviously more relaxed and did not require much structuring or deeper review. We asked meeting groups the following questions, based on the general principles of effective meetings:
• Do meetings have a pre-circulated agenda? This indicates a purpose for the meeting and provides participants with subject matter they may investigate for debate or presentment.
• Is a chair or leader appointed? Evidence there will be a ‘controller’ to focus attendees on agenda items under discussion, assign actions to specific individuals where necessary, and ‘watch the clock’ so items are not left undecided.
The importance of formally deferring items (developing a ‘deferred items’ list) that may not have been discussed due to time delays or excessive discussion was highlighted to ensure they are carried forward to the next meeting.
• Are desired outcomes or decision options understood? Where applicable, this ensures participants are aware a decision is required for certain discussion items and staff should be prepared to voice personal views on various topics.
• Are meetings properly ‘time planned’? This suggests thought has been given to adequacy of time required to do justice to each topic by ‘guesstimating’ the approximate amount of time required to
address each agenda item.
• Is relevant pre-reading circulated? Where an item warrants it, pre-reading affords attendees an opportunity to prepare and contribute more meaningfully, also evidencing thoroughness of the meeting coordinator.
• Are self-assessment ‘meeting evaluations’ conducted? Means by which teams strive to improve meeting quality and outcomes, such as valuable ‘feedback’ for the chair or meeting leader.
• Are minutes (including agreed resolutions) and ‘action istems’ documented and distributed? This provides continuity and implementation of resolutions when minutes are tabled at subsequent meetings. Of course, such minutes should be reviewed and accepted by the meeting leader to ensure they are an accurate reflection of the group’s discussions. Matters that may have been discussed casually, and even agreed, after the meeting should not be recorded in minutes but held over for the agenda of the next formal meeting.
Staff, clinicians and principals found the exercise beneficial, injecting meaningful structure and achievement-oriented content into meetings, without introducing excessive bureaucracy. We also suggested occasional (not just customary annual) rotation of meeting leaders to spread valuable experience.
While meetings are a useful form of communication, decision making and planning, the other extreme is too many meetings; meetings for the sake of meetings (refer the infamous John Cleese skit, ‘Meetings, meetings, bloody meetings”).
A decision that could be made easily by circulated email might only require a meeting if parties involved cannot reach agreement on a proposal or the matter is sufficiently important to deserve a formal meeting.
ABOUT THE AUTHOR: Karen Crouch is managing director of Health Practice Creations Group, a company that assists with practice set ups, administrative, legal and financial management of practices. Contact Karen on 0433 233 478, [email protected] or visit www.hpcgroup.com.au.
BELOW: It’s quality and results of meetings, rather than the number of meetings, that ultimately counts, says Karen Crouch.
Image: Karen Crouch
Image: Jacob Lund/shutterstock.com.
SOAPBOX
DIABETES-RELATED HEARING LOSS

the body cannot effectively use the insulin it produces.
The World Health Organization reports a staggering 537 million individuals between the ages of 20 to 79 are living with diabetes. In Australia alone, the prevalence has doubled since 1981, with one in 20 Australians diagnosed with the condition. Type 2 diabetes accounts for the majority of cases, affecting 87.6% of those with diabetes. Additionally, Indigenous populations face a significantly higher risk.
Links to hearing loss
Recent studies have shed light on the connection between diabetes and hearing loss. High blood sugar levels in people with diabetes can disrupt the auditory system, leading to physiological and anatomical changes.
Research indicates that individuals with diabetes are at a moderate to high risk of experiencing hearing loss, particularly sensorineural hearing loss (SNHL).
Studies have also shown a correlation between the duration of diabetes and the incidence of hearing loss, with longer-standing diabetes posing a higher risk.
Additionally, poor glycaemic control exacerbates this risk and individuals demonstrating higher HbA1c (glycated

Understanding the factors
Factors such as poor glycaemic control, duration of diabetes, and metabolic abnormalities contribute to the development and progression of hearing loss in people with diabetes.
Studies have found a significant association between elevated HbA1c levels and an increased risk of hearing impairment. Furthermore, individuals with long-standing diabetes are more likely to experience damage to cochlear hair cells, particularly at high frequencies.
Examining glycaemic control
Glycaemic control, as measured by HbA1c levels, plays a crucial role in managing diabetes-related complications, including hearing loss.
While some studies suggest a positive correlation between glycaemic control and hearing preservation, others yield inconclusive results. Research investigating the effect of glycaemic control on hearing recovery post-insulin treatment presents mixed findings, indicating the need for further exploration.
Future directions
Despite advances in understanding diabetes-related hearing loss, there
identification and intervention strategies, ultimately improving health outcomes and quality of life for individuals living with diabetes.
Future studies focusing on the influence of early glycaemic control on hearing loss progression in specific populations, such as Indigenous Australians, are warranted to inform targeted interventions and enhance overall health outcomes. By raising awareness of the link between diabetes and hearing loss and advocating for further research, we can work towards mitigating the impact of this debilitating complication and improving the lives of those affected.
NOTE: References will appear in the online version of this article.
Name: Lian Gijo
Qualifications: Bachelor’s degree in Audiology and Speech Language Pathology from India’s Manipal Academy of Higher Education, and a Master’s in Clinical Audiology from Macquarie University.
Affiliations: Audiology trainer with the Australasian College of Audiometry.
Location: Sydney Years in industry: Five
“HIGH
BLOOD SUGAR LEVELS IN PEOPLE WITH DIABETES CAN DISRUPT THE AUDITORY SYSTEM, LEADING TO PHYSIOLOGICAL AND ANATOMICAL CHANGES.”
Recent studies have shed light on the connection between diabetes and hearing loss.
Factors such as poor glycaemic control can contribute to the development and progression of hearing loss in people with diabetes.
Lian Gijo
Image: Proxima
Image:
Lian Gijo.
People on the move

Mr James Chapman brings a wealth of experience to this role, having joined Specsavers in 2020 as an audiology relationship manager. Over the past four years, he has made a positive impact and created great inroads in supporting and strengthening its partners. Most recently, he has been on secondment as the senior professional recruitment manager,
Specsavers. In his new role, Chapman is responsible for strategic planning and implementation of Specsavers Audiology’s growth activity for Australia and New Zealand as Specsavers Audiology continues to grow its footprint across both countries.





neurotology. She previously worked at the University of Pretoria, South Africa performing a multi-functional role including lecturing, clinical work and research. Dr Heinze has authored various publications and has presented internationally. in May 2024.
EVENTS CALENDAR
To list an event in our calender, email editor,

23 October.
AUGUST 2024
COCHLEAR AND AUDIOLOGY AUSTRALIA
Connect on cochlear implant care Macquarie University 9 August audiology.asn.au
OMOZ (OTITIS MEDIA AUSTRALIA) 2024
Newcastle, Australia 27-30 August Omoz.com.au
EAR HEALTH COURSE
Cerumen management 101 Flinders University, Adelaide 24 August earhealthcourses.com.au
SEPTEMBER 2024
36TH WCA WORLD CONGRESS OF AUDIOLOGY Paris, France 19-22 September 2024 wca2024paris.com
OCTOBER 2024
ORL'24
New Zealand Society of Otolaryngology – Head and Neck Surgery 77th annual general and scientific meeting Hamilton, New Zealand 15-18 October orl24.nz
INDEPENDENT AUDIOLOGISTS
AUSTRALIA
Audiology for life seminar Melbourne, Australia 11 October independentaudiologists.net.au

OCTOBER 2024
NEXTSENSE AUDIOLOGY MASTERCLASS
Vestibular function and balance performance in children with sensorineural hearing loss
Online 23 October Nextsense.org.au
NOVEMBER 2024
NFMRI
National Foundation for Medical Research and Innovation research with purpose conference Moreton Island, Australia 28 November eventbrite.com.au
DECEMBER
NEXTSENSE
2024
Learning day for itinerant teachers of the deaf Australian Hearing Hub Macquarie University 6 December Nextsense.org.au
MARCH 2025
ASOHNS 2025
Annual scientific meeting Sydney, Australia 28-30 March asohns.arinex.one/

NextSense will run an online audiology class on vestibular function and balance performance in children with sensorineural hearing loss on
ORL'24, the New Zealand Society of Otolaryngology-Head and Neck Surgery's 77th annual general and scientific meeting, will be in Hamilton from 15-18 October.
A medical research and innovation conference will be on Moreton Island, Queensland, on 28 November.